Panax Ginseng Complete Research Review
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Panax ginseng may interact with anticoagulant medications (warfarin, aspirin), antidepressants, MAO inhibitors, stimulants, antidiabetic drugs, and immunosuppressants. Individuals with bipolar disorder, hormone-sensitive cancers, or autoimmune conditions should exercise caution. Consult a qualified healthcare provider before beginning any supplementation protocol.
Panax Ginseng: Complete Evidence-Based Review, Dosing, and Protocol Guide
The most historically used cognitive enhancer in the world, with genuine acute and chronic RCT evidence — and a research record more nuanced than most sources acknowledge. What the clinical trials actually show, who benefits most, and where it fits in a serious nootropic protocol.
Bottom Line — For Those Who Want It First
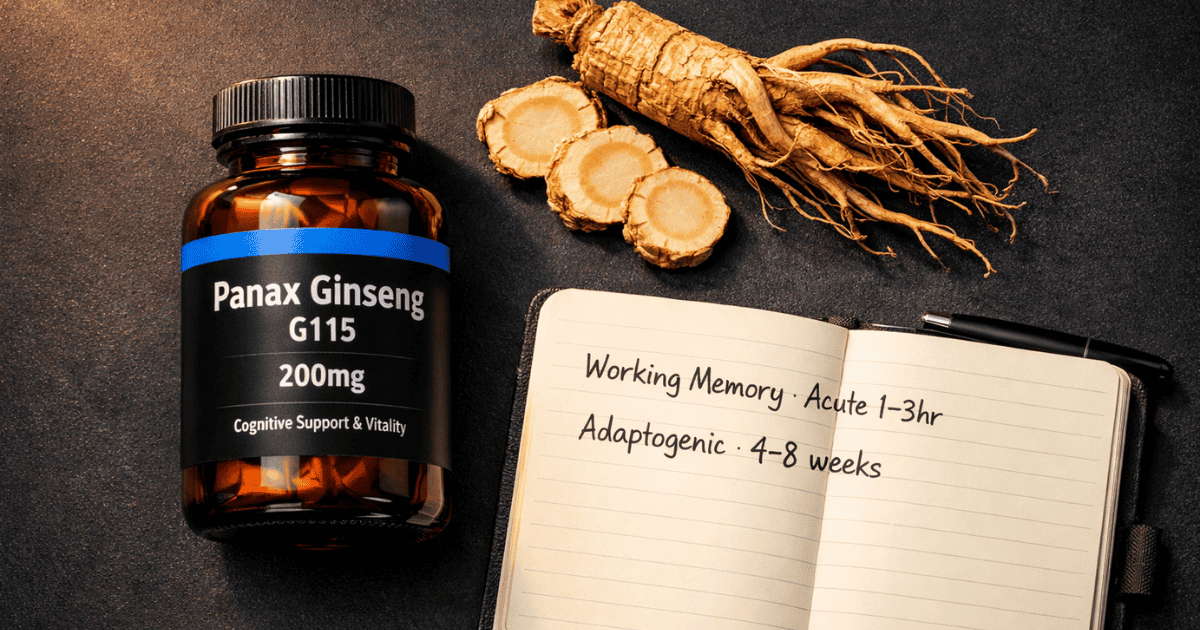
Panax ginseng has documented acute cognitive effects — primarily working memory and mental fatigue reduction — at doses of 200–400mg, with evidence emerging within 1–3 hours of administration. Chronic use adds a slower adaptogenic layer: HPA normalization, anti-fatigue support, and neuroprotection. A 2024 meta-analysis of 15 RCTs confirmed significant memory improvement, but null results for attention and executive function. The honest picture is a compound with real and specific effects, strongest in individuals under cognitive load or stress, and best positioned as the activating adaptogen in a stack that already includes foundational compounds.
Standard Protocol
200–400mg G115 standardized extract
Onset Timeline
Acute: 1–3 hours · Adaptogenic: 4–8 weeks
Evidence Level
15 RCTs · 2024 meta-analysis
Key Caution
Warfarin, antidepressants, bipolar disorder
What Panax Ginseng Is — Two Species, One Name, Very Different Profiles
Few compounds in the nootropics literature have a longer documented history than ginseng. Used in traditional Chinese and Korean medicine for over 2,000 years as a general tonic for vitality, mental clarity, and stress resilience, Panax ginseng is now one of the most commercially widespread supplements globally — and one of the most frequently misunderstood. The most important clarification to make before reviewing the evidence: “ginseng” is not a single compound. There are two distinct species with meaningfully different ginsenoside profiles and clinical evidence bases, and the distinction matters for anyone building a serious protocol.
Asian ginseng (Panax ginseng C.A. Meyer) — also called Korean ginseng — is the most extensively researched species. It contains a complex profile of over 30 ginsenosides, with Rb1, Rg1, Re, Rd, and Rg3 most studied. The ratio of Panaxatriol to Panaxadiol ginsenosides is relatively balanced. Its effects are generally described as warming and activating — increased energy, improved focus, enhanced stress resilience. The majority of the clinical trial base for cognitive effects uses G115, a standardized Panax ginseng extract containing 4% total ginsenosides.
American ginseng (Panax quinquefolius) has a distinctly higher ratio of Panaxadiol to Panaxatriol ginsenosides. This different profile produces a pharmacologically different effect: cooler, calmer, less stimulating than Asian ginseng, with a particularly strong signal in working memory research. The extract Cereboost (standardized to 10.65% ginsenosides) has been specifically used in working memory RCTs in healthy adults with consistent positive results. If working memory in healthy, non-stressed individuals is your primary target, American ginseng has the stronger evidence for that specific application.
This review covers both species where the evidence warrants, but prioritizes Asian ginseng (G115) as the primary recommendation for the adaptogenic + cognitive performance application that most readers of nootropic beginners guides are pursuing. The sourcing section specifies both options and when each is appropriate.
The Mechanisms: How Ginsenosides Work in the Brain
Ginseng’s cognitive effects operate through multiple overlapping mechanisms — a complexity that makes it genuinely useful across several cognitive domains, but also makes it harder to attribute effects to any single pathway. The four most well-characterized mechanisms relevant to cognitive performance are as follows.
1. Nitric Oxide–Mediated Cerebral Blood Flow
The most well-supported acute mechanism for ginseng’s cognitive effects is nitric oxide (NO) synthase activation by Panaxatriol ginsenosides, particularly ginsenoside Rg1. NO is a potent vasodilator — its release from endothelial cells increases cerebral blood flow, delivering more glucose and oxygen to metabolically active brain tissue. This mechanism is dose-dependent and ginsenoside-profile dependent: the Panaxatriol ginsenosides in Asian ginseng (and particularly in Cereboost’s high-Panaxatriol American ginseng extract) drive stronger NO-mediated effects than Panaxadiol-dominant profiles. The practical implication is that ginseng’s acute cognitive effects are partly vascular — the same mechanism through which exercise acutely improves cognitive performance, mediated here by a ginsenoside-triggered molecular pathway rather than mechanical cardiac output.
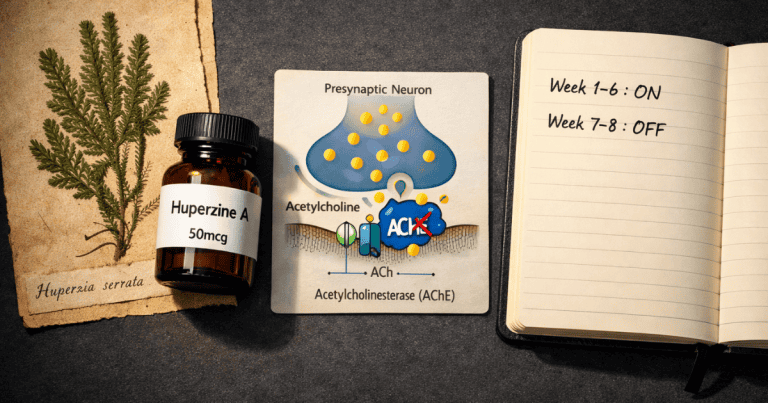
2. Cholinergic Enhancement
Ginsenosides increase both choline uptake into neurons and acetylcholine release at synaptic terminals. This cholinergic effect partially overlaps with the mechanism targeted by Alpha-GPC — both increase the substrate availability and release rates of acetylcholine in circuits governing working memory, attention, and hippocampal learning. The ginseng cholinergic effect is less direct than Alpha-GPC’s pure substrate delivery, but it operates alongside the vascular mechanism described above, producing a combined effect on cholinergic cognitive function that neither mechanism alone fully explains. The acetylcholinesterase inhibition observed with some ginsenosides adds a third layer — slowing ACh breakdown in addition to increasing its synthesis and release.
3. HPA Axis Modulation and Glycoregulation
Like Ashwagandha, ginseng exerts adaptogenic effects on the HPA axis — reducing stress-induced corticosterone elevation and normalizing HPA reactivity under chronic stress. However, ginseng’s adaptogenic mechanism is pharmacologically distinct from Ashwagandha’s. Where Ashwagandha primarily modulates glucocorticoid receptor sensitivity and CRH signaling, ginsenosides appear to act through NO-mediated inhibition of HPA stress responses and direct effects on adrenocortical function. Importantly, ginseng also has consistent glycoregulatory effects — multiple studies document that ginsenosides reduce blood glucose levels through enhanced insulin sensitivity, with Reay and colleagues (2005) finding significant blood glucose reduction alongside cognitive performance improvements during sustained mentally demanding tasks. This glucose-stabilizing effect likely contributes to sustained cognitive performance by reducing the blood glucose instability that impairs prefrontal function during prolonged demanding work.
4. Neuroprotection and Synaptic Plasticity
At the longer timescale relevant to chronic supplementation, ginsenosides demonstrate meaningful neuroprotective effects through anti-inflammatory, antioxidant, and anti-apoptotic mechanisms. Ginsenoside Rb1 reduces oxidative stress and neuroinflammation through multiple signaling pathways. Ginsenoside Rg1 protects dopaminergic neurons, modulates BDNF expression, and supports hippocampal long-term potentiation. Ginsenoside Rg3 modulates NMDA receptor activity — at the concentration ranges achievable through standard supplementation, this appears to be a nuanced regulatory effect on hippocampal LTP rather than the excitotoxic NMDA blockade seen in vitro at very high concentrations. The brain health and longevity case for ginseng is as strong as the acute performance case — population studies show that 5+ years of consistent ginseng consumption correlates with reduced cognitive decline and mortality, though causality in epidemiological data is always cautious.
The Research: What the Clinical Trials Actually Show
Ginseng’s cognitive research base is substantial but requires careful reading. Enthusiastic marketing claims — “ancient mental performance secret” — coexist with a meta-analytic literature that shows both real effects and important null results. Both are true, and understanding which domains are genuinely supported and which are not is the foundation for using it correctly.
The 2024 Meta-Analysis: Memory Yes, Attention No
The most comprehensive systematic review of ginseng’s cognitive effects published to date, synthesized 15 randomized controlled trials with 671 total participants — including healthy adults, those with mild cognitive impairment, schizophrenia, and Alzheimer’s disease. The findings are specific and deserve precise presentation rather than the vague summaries that typically circulate.
Memory improvement was statistically significant (SMD = 0.19, 95% CI: 0.02–0.36, p < 0.05). At high doses, the memory effect size was larger (SMD = 0.33, 95% CI: 0.04–0.61, p < 0.05) — a meaningful dose-response relationship. Overall cognition, attention, and executive function did not show statistically significant improvement (all p-values > 0.05). This is an important result, not a reason to dismiss ginseng. Memory is the cognitive domain most tightly linked to the cholinergic and vascular mechanisms described above. The null results for attention and executive function suggest ginseng is a specific compound for specific cognitive targets — not a broad cognitive enhancer that improves everything simultaneously.
Acute Effects: The Reay and Kennedy Studies
The acute cognitive effects of Panax ginseng have been characterized through a series of crossover studies by Reay, Kennedy, and Scholey. A 2005 study found that a single 200mg dose of G115 significantly improved Serial Sevens performance — a demanding serial subtraction task measuring working memory under sustained cognitive load — and reduced mental fatigue ratings during the test period, while also producing significant blood glucose reduction compared to placebo. A follow-up study replicated the Serial Sevens finding and extended it to Serial Threes, alongside improvements on the Rapid Visual Information Processing task. In a dose-comparison study, 400mg significantly improved Quality of Memory and Secondary Memory scores at all post-dose timepoints. The consistent pattern across these acute studies: ginseng’s effects are most pronounced during sustained cognitively demanding tasks — conditions of high cognitive load where both the cholinergic demand and the glucose utilization rate are elevated — rather than in resting assessments.
Working Memory in Healthy Adults: The Cereboost Studies
The Cereboost extract of American ginseng has produced consistent working memory improvements across two well-designed crossover trials in healthy adults. The first study (N = 32, healthy young adults) found significant working memory improvements at 200mg at the 1-hour and 6-hour assessment points. The replication study (N = 52, healthy middle-aged adults aged 40–60, mean age 51.6) confirmed working memory improvement at 3 hours post-dose — extending the finding from young to middle-aged populations. The middle-aged study is particularly relevant because memory consolidation and retrieval processes begin to decline in this age range, making them a more appropriate target population than young adults for whom the effect size was smaller. The 200mg Cereboost dose producing working memory improvements in healthy middle-aged adults is one of the more robust specific findings in the entire ginseng cognitive literature.
Chronic Use in MCI and Alzheimer’s Populations
For those interested in long-term neuroprotective use — the brain health longevity angle — the chronic evidence in impaired populations is notable. Park and colleagues (2019) conducted a 6-month randomized double-blind placebo-controlled trial in 90 Korean volunteers with mild cognitive impairment. At 3g daily, Panax ginseng produced significant improvements on the Rey Complex Figure Test immediate and 20-minute delayed recall versus placebo — a demanding episodic memory assessment. Lee and colleagues (2008) found that 4.5g daily Panax ginseng over 12 weeks significantly improved both MMSE and ADAS-cognitive subscale scores in Alzheimer’s disease patients versus control, with gains declining back toward baseline after discontinuation — establishing both efficacy and reversibility, the latter confirming the effect was compound-dependent rather than spontaneous improvement. These studies use doses (3–4.5g) substantially above the typical acute cognitive enhancement range (200–400mg), suggesting a dose-response relationship where higher chronic doses produce different magnitude effects than acute lower doses in different populations.
The Honest Summary of the Evidence
Ginseng has genuine, replicated, dose-dependent cognitive effects concentrated in the memory domain — particularly working memory and episodic recall during sustained demanding tasks. These effects are strongest in populations under cognitive load, those with pre-existing memory impairment, and middle-aged adults whose cholinergic and vascular cognitive substrate is naturally beginning to decline. Attention and executive function show null results in the meta-analytic evidence, which means ginseng is not the right primary compound for pure focus enhancement. Ashwagandha addresses HPA-driven cortisol erosion; ginseng addresses a different cluster — vascular delivery, cholinergic substrate, memory consolidation, and glycoregulation during demanding cognitive work. These are complementary targets, not redundant ones.
Dosing Protocol: G115, Cereboost, and the Dose-Response Relationship
The dose-response relationship for ginseng is not linear and involves non-obvious patterns that the research reveals clearly. Understanding this prevents the common mistake of assuming more is always better.
Asian Ginseng (G115) — Cognitive Performance Protocol
The dose-response non-linearity in the Kennedy/Scholey studies is worth noting: 200mg and 400mg both produced memory improvements, but 600mg slowed Speed of Attention — a reaction-time measure — at some assessment points. The current interpretation is that very high acute doses produce a mild calming or slowing effect through GABAergic or adenosine-related mechanisms that partially offsets the cognitive performance benefit. This is not dangerous, but it means that more ginseng is not better acutely. The 200–400mg range is well-defined by the evidence; do not exceed 400mg for acute sessions.
American Ginseng (Cereboost) — Working Memory Protocol
If working memory is the primary target — particularly for those aged 40+ who notice early memory consolidation changes — Cereboost at 200mg is the most directly supported option in the literature. It is calmer in its effect profile than G115, does not produce the occasional stimulatory edge that some users report with Asian ginseng, and has been specifically validated in the middle-aged population most likely to benefit. 200mg once daily in the morning or 60–90 minutes before cognitively demanding sessions is the protocol the research supports.
Cycling: Why It Is Required for Ginseng
Unlike Ashwagandha, where cycling is recommended but not required for tolerance management, cycling is strongly recommended for ginseng based on both traditional usage patterns and the pharmacological rationale. Most practitioners and the traditional Panax ginseng literature recommend 2–3 months on followed by 3–4 weeks off. Two mechanisms support this: first, ginseng’s HPA modulation involves adrenocortical interaction, and prolonged continuous use may reduce adrenal sensitivity in ways that diminish the adaptogenic response — a break restores baseline reactivity; second, the activating properties of ginseng can accumulate into chronic overstimulation in sensitive individuals, particularly those also using caffeine. The Korean tradition of seasonal ginseng use — autumn and winter, with spring and summer breaks — reflects millennia of empirical observation of this pattern. The modern protocol: 8–12 weeks on, 3–4 weeks off, then repeat.
⬇ Free Download
Get the 7-Day Brain Optimization Protocol
The evidence-based behavioral and supplement framework for your first week of cognitive enhancement — covering sleep optimization, L-theanine + caffeine, creatine, Lion’s Mane, and the daily protocols that make them work. Completely free.
Join 2,000+ readers optimizing their cognitive performance. No spam, ever. Unsubscribe anytime.
Timing Protocol: When to Take It and What to Expect
Ginseng has two distinct timing considerations that depend on whether you are using it for acute cognitive performance or chronic adaptogenic support — and these are not in conflict.
Timing Framework
Morning (upon waking or with breakfast): Daily adaptogenic + chronic neuroprotective use. Consistent daily timing matters more than the exact clock time for the cumulative adaptogenic effect.
60–90 minutes before demanding cognitive work: For the acute working memory and anti-fatigue effects. Ginseng peaks in blood concentration at approximately 1–3 hours post-dose — time intake accordingly to coincide with the start of your primary cognitive session.
Avoid after 2pm: Ginseng’s activating properties can delay sleep onset in sensitive individuals. Unlike Ashwagandha — which has a morning and evening split dosing protocol — ginseng should be kept entirely within the first half of the day.
What to Expect — Onset Timeline
Ginseng’s timeline is dual-phase in a way that no other adaptogen covered in this series replicates exactly. The acute effects — working memory, mental fatigue reduction, blood glucose stability during demanding tasks — are present within the first dose and peak at 1–3 hours. These effects are real and repeatable, but they are subtle compared to caffeine. Ginseng does not produce a noticeable alertness kick. What it produces is smoother, sustained cognitive output that degrades more slowly over a demanding session than unaugmented baseline.
The adaptogenic layer builds over 4–8 weeks of consistent daily use — HPA normalization, improved stress resilience, and the more pronounced memory effects observed in chronic trials. The practical experience: in weeks 1–2, the primary observable effect is smoother cognitive performance during demanding sessions. By weeks 4–6, the adaptogenic benefits are established, and users typically report clearer cognitive baselines with less day-to-day variability driven by stress. The 12-week mark is the appropriate assessment point for the full chronic effect profile.
Safety, Contraindications, and Drug Interactions
Panax ginseng has a well-characterized safety profile with a small number of significant interactions and contraindications that require direct discussion. The general population safety record is strong — it has been consumed by hundreds of millions of people over millennia without systematic toxicity signals. The specific interaction risks, however, are real and clinically important.
Anticoagulant Interaction — Most Clinically Significant
Ginsenosides have demonstrated antiplatelet effects and may enhance the anticoagulant action of warfarin (Coumadin) through CYP450 enzyme interaction — specifically CYP2C9, which metabolizes warfarin. Case reports of elevated INR in warfarin patients using ginseng exist in the pharmacovigilance literature. Anyone taking warfarin, heparin, aspirin at anticoagulant doses, or other blood-thinning medications must discuss ginseng with their prescribing physician before use. This is a category-level contraindication, not a theoretical one.
Antidepressants and MAO Inhibitors
Ginseng’s monoamine modulation — particularly its effects on dopamine and serotonin — creates potential pharmacodynamic interactions with antidepressant medications. With MAO inhibitors specifically, the interaction risk is heightened: case reports describe manic-like episodes and agitation in patients combining ginseng with phenelzine. With SSRIs, the interaction is less well-documented but pharmacologically plausible through additive serotonergic effects. Anyone taking prescription antidepressants should not add ginseng without explicit prescriber guidance.
Bipolar Disorder — Significant Caution Required
Ginseng’s activating and monoamine-modulating properties carry documented risk of triggering or worsening manic episodes in individuals with bipolar disorder. This is not a theoretical concern — it appears directly in the clinical contraindication literature and should be treated as an absolute contraindication in this population. Individuals with bipolar disorder should not use ginseng.
Blood Glucose Interactions
The glycoregulatory effects of ginsenosides — well-documented and generally beneficial for cognitive performance — become a pharmacodynamic interaction concern in individuals taking antidiabetic medications (insulin, metformin, sulfonylureas). Additive blood glucose lowering can produce hypoglycemia. Anyone with type 1 or type 2 diabetes being pharmacologically managed should monitor blood glucose carefully and consult their physician before adding ginseng. For individuals without diabetes, the glucose-stabilizing effect is a meaningful benefit, not a risk.
Ginseng Abuse Syndrome — Dose-Dependent Overstimulation
At very high doses and with prolonged continuous use, Panax ginseng can produce a cluster of symptoms described as “ginseng abuse syndrome” in the older literature: hypertension, insomnia, morning diarrhea, skin rash, and restlessness. This was documented primarily with doses significantly above therapeutic range and without cycling. At the 200–400mg G115 range with proper cycling, this risk is negligible. It is mentioned because it illustrates why the “more is better” approach to ginseng — sometimes encountered among biohackers — is pharmacologically incorrect.
⚠ Contraindications Summary
Avoid entirely: Bipolar disorder, warfarin or other anticoagulant therapy, MAO inhibitors, pregnancy, upcoming surgery within 2 weeks (antiplatelet effects), hormone-sensitive cancers.
Discuss with prescriber first: Antidepressants (SSRIs, SNRIs), antidiabetic medications, immunosuppressants, stimulant medications, antihypertensives.
Sourcing: What to Look For and Why Generic Ginseng Is Not Adequate
Ginseng quality is highly variable in the commercial supplement market. Unlike Ashwagandha — where the KSM-66 and Sensoril branded extracts provide clear standardization benchmarks — generic ginseng products use terms like “standardized Panax ginseng root extract” without specifying ginsenoside content, extraction method, or ginsenoside profile. ConsumerLab testing has repeatedly identified ginseng products that contain significantly less ginsenoside content than claimed. Given that the cognitive evidence is tied to specific extract standards and ginsenoside concentrations, this matters practically.
G115 (Panax ginseng): The extract used in the Reay, Kennedy, and Scholey studies that established the cognitive performance evidence base. Standardized to 4% total ginsenosides using a defined extraction protocol. This is the benchmark for the acute cognitive performance and adaptogenic applications. Products listing G115 on the label and providing third-party testing documentation are the appropriate choice for the cognitive performance application described in this guide.
Cereboost (Panax quinquefolius): The American ginseng extract standardized to 10.65% ginsenosides and validated in the working memory RCTs. If working memory in healthy middle-aged adults is the primary target, this is the more specifically supported option. Products listing Cereboost on the label and providing a certificate of analysis are the appropriate choice.
What to avoid: unspecified “ginseng root extract” without named branded extract or ginsenoside percentage; products with no third-party testing; products listing only “root powder” without extraction specification; anything not specifying the species (Panax ginseng vs. Panax quinquefolius are not interchangeable). A COA confirming ginsenoside content is non-negotiable for a compound where product variability is this well-documented.
Stack Integration: Where Ginseng Fits and How It Relates to Ashwagandha
The question most readers of the Ashwagandha guide will have arriving at this article is: how do these two adaptogens relate, and should I use one or both? The answer is both, but sequentially and for different reasons.
Ashwagandha is the cortisol and stress architecture compound. Its primary targets are HPA axis normalization, chronic cortisol reduction, sleep architecture, and the removal of the stress-driven cognitive erosion that degrades baseline performance over time. It works slowly and cumulatively, with no meaningful acute cognitive effects. It belongs in a protocol as infrastructure.
Ginseng addresses a different cluster: vascular cerebral delivery, cholinergic substrate availability, working memory and episodic recall during demanding sessions, blood glucose stability during sustained cognitive work, and dopaminergic/serotonergic tone. It has both acute and chronic effects. It is more activating than Ashwagandha. It pairs well with the L-theanine + caffeine stack specifically because caffeine increases ACh demand (which ginseng’s cholinergic mechanism partially addresses) and because the glycoregulatory effect of ginseng complements caffeine’s tendency to elevate blood glucose transiently in some users.
The recommended sequencing: establish Ashwagandha first (weeks 1–8), assess cognitive baseline improvement from HPA normalization, then introduce ginseng as the second adaptogen layer. This sequencing allows you to attribute effects correctly rather than adding both simultaneously and having no clear picture of what is doing what. After both are established, the combined profile — cortisol architecture (Ashwagandha) + vascular/cholinergic/working memory support (ginseng) + acute focus layer (L-theanine + caffeine) — covers the primary determinants of sustained high cognitive performance under real-world conditions.
Integrated Morning Stack Protocol
On waking
Ginseng 200–400mg (G115 or Cereboost) with water
60 min after waking
Caffeine 100mg + L-Theanine 200mg
With breakfast
Lion’s Mane 1000mg + Creatine 5g + DHA 1000–2000mg
Evening
Ashwagandha 300–600mg KSM-66 + Magnesium L-Threonate 1500mg
Frequently Asked Questions About Panax Ginseng
How long does Panax ginseng take to work?
Ginseng has two distinct timeframes. Acute effects — working memory support, mental fatigue reduction, blood glucose stabilization during demanding tasks — are present within the first dose and peak at 1–3 hours post-administration. These are subtle compared to caffeine: not a noticeable alertness surge, but smoother and more sustained cognitive output during demanding sessions. The chronic adaptogenic effects — HPA normalization, baseline stress resilience, more pronounced memory improvements — build over 4–8 weeks of consistent daily use, with the full profile established by week 12.
What is the difference between Panax ginseng and American ginseng?
The two species have different ginsenoside profiles — the ratio of Panaxatriol to Panaxadiol ginsenosides differs substantially — which produces meaningfully different effects. Asian ginseng (Panax ginseng, extract G115) is more activating: stronger energy and stress-resilience effects, more pronounced adaptogenic profile. American ginseng (Panax quinquefolius, extract Cereboost) is calmer, less stimulating, and has the stronger clinical evidence base specifically for working memory in healthy adults. For cognitive performance in stressed individuals or as a general adaptogen, Asian ginseng is the default recommendation. For isolated working memory support in healthy middle-aged adults who are sensitive to stimulation, Cereboost at 200mg is the more targeted choice.
Can I take Panax ginseng with Ashwagandha?
Yes, and for most people who benefit from both, combining them is appropriate — with the important caveat of sequencing. Establish Ashwagandha first for 6–8 weeks to normalize HPA function and assess its contribution, then introduce ginseng. Both are adaptogens, but their mechanisms are complementary rather than redundant: Ashwagandha targets cortisol and HPA stress architecture; ginseng targets vascular delivery, cholinergic substrate, working memory, and glycoregulation. No clinically significant adverse interaction has been documented between the two compounds at standard doses. The most important timing distinction: Ashwagandha is split morning and evening; ginseng is taken in the morning only.
Does Panax ginseng need to be cycled?
Yes — cycling is recommended more strongly for ginseng than for most other adaptogens in this series. The standard protocol is 8–12 weeks of daily use followed by a 3–4 week break, then repeat. Two reasons support this: first, ginseng’s HPA interaction involves adrenocortical function, and prolonged continuous exposure may reduce adrenal responsiveness in ways that blunt the adaptogenic effect over time — a break restores baseline sensitivity; second, ginseng’s activating properties can accumulate into chronic overstimulation in sensitive individuals, particularly those using caffeine regularly. This cycling pattern also mirrors the traditional Panax ginseng usage pattern documented in Korean and Chinese medicine over centuries.
Is Panax ginseng safe for long-term use?
At recommended doses (200–400mg G115 standardized extract) with proper cycling, Panax ginseng has a well-established safety record supported by both the clinical trial literature and centuries of human consumption. The primary safety considerations are pharmacodynamic: interactions with anticoagulants (warfarin), antidepressants, MAO inhibitors, and antidiabetic medications — not direct toxicity of ginseng itself in healthy individuals without these medications. The “ginseng abuse syndrome” pattern documented in older literature occurred with doses significantly above the standard cognitive performance range and without cycling breaks. With proper cycling and at standard doses, long-term use appears safe for healthy adults without the contraindicated medications or conditions described in this guide.
Scientific References
- Chen, T., et al. (2024). Effects of Ginseng on Cognitive Function: A Systematic Review and Meta-Analysis. Phytotherapy Research. Wiley
- Reay, J.L., Kennedy, D.O., Scholey, A.B. (2005). Single doses of Panax ginseng (G115) reduce blood glucose levels and improve cognitive performance during sustained mental activity. Journal of Psychopharmacology, 19(4), 357–365. PubMed
- Scholey, A., et al. (2010). Effects of American ginseng (Panax quinquefolius) on neurocognitive function: an acute, randomised, double-blind, placebo-controlled, crossover study. Psychopharmacology, 212(3), 345–356. PMC
- Ossoukhova, A., et al. (2015). Improved working memory performance following administration of a single dose of American ginseng (Panax quinquefolius L.) to healthy middle-age adults. Human Psychopharmacology, 30(2), 108–122. PubMed
- Park, K.C., et al. (2019). Cognition enhancing effect of Panax ginseng in Korean volunteers with mild cognitive impairment: a randomized, double-blind, placebo-controlled clinical trial. Translational and Clinical Pharmacology, 27(3), 92–97. PMC
- Lee, S.T., et al. (2008). Panax ginseng enhances cognitive performance in Alzheimer disease. Alzheimer Disease and Associated Disorders, 22(3), 222–226. PubMed
- Kim, S., et al. (2002). Inhibitory effect of ginsenosides on NMDA receptor-mediated signals in rat hippocampal neurons. Biochemical and Biophysical Research Communications, 296(2), 247–254. PubMed
- Reay, J.L., Kennedy, D.O., Scholey, A.B. (2006). Effects of Panax ginseng, consumed with and without glucose, on blood glucose levels and cognitive performance during sustained ‘mentally demanding’ tasks. Journal of Psychopharmacology, 20(6), 771–781. PubMed
- Nah, S.Y., et al. (2024). Emerging evidence that ginseng components improve cognition in subjective memory impairment, mild cognitive impairment, and early Alzheimer’s disease. Journal of Ginseng Research. PMC
- Hemmati, A.A., et al. (2025). The role of Panax ginseng in neurodegenerative disorders: mechanisms, benefits, and future directions. BMC Complementary Medicine and Therapies. PubMed