Ashwagandha Complete Research Review
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning any supplementation protocol — particularly if you have thyroid conditions, autoimmune disorders, liver disease, are pregnant, or take any medications including antidiabetics, antihypertensives, immunosuppressants, sedatives, or thyroid hormone medications. Individual responses vary significantly.
Ashwagandha: Complete Evidence-Based Review, Dosing, and Protocol Guide
The most-researched adaptogen in the nootropic literature. What the clinical trials actually show about cortisol, cognition, and sleep — and who should not use it. An honest evaluation after 18+ years of personal testing.
Bottom Line — For Those Who Want It First
Ashwagandha is the strongest-evidenced adaptogen available for stress and cortisol reduction, with a growing body of RCT data supporting cognitive benefits — particularly memory, attention, and information processing speed. Crucially, these are not acute effects. Ashwagandha builds over 4–8 weeks and works primarily through the HPA axis, not through direct stimulation. It is not a replacement for an acute focus stack. It is foundational infrastructure for anyone operating under chronic stress whose cognitive performance is being degraded from the inside out.
Standard Protocol
300–600mg KSM-66 daily
Onset Timeline
4–8 weeks for full effect
Evidence Level
Multiple RCTs · 2 meta-analyses
Key Caution
Thyroid, autoimmune, liver disease
What Ashwagandha Actually Is — And Why Cognitive Enhancers Should Care
The majority of nootropics covered in the Nootropics & Supplements Guide work on cognitive performance through direct neurochemical mechanisms — enhancing acetylcholine, modulating dopamine, promoting alpha waves. Ashwagandha takes a fundamentally different approach, and understanding that difference is the key to using it correctly. It doesn’t directly boost neurotransmitters associated with focus or memory. It removes the primary system-level obstacle that prevents your cognitive capacity from expressing itself: chronic physiological stress.
Ashwagandha (Withania somnifera) is a small shrub native to India, North Africa, and the Mediterranean. Its roots have been used in Ayurvedic medicine for over 3,000 years as a “rasayana” — a rejuvenating compound meant to promote longevity, vitality, and mental clarity. The modern research literature has largely validated the stress-reduction claims, and is accumulating solid evidence for direct cognitive effects in stressed populations. It belongs to a category of compounds called adaptogens — substances that increase the body’s resistance to physical, chemical, and biological stressors. In the best nootropics for beginners guide, it makes the list precisely because of this foundational role — it’s rarely the most dramatic compound in a stack, but it’s often doing the most important structural work.
Through 18+ years of working with people on cognitive protocols, the pattern I observe repeatedly is this: high-performing individuals under significant chronic stress who add stimulants and focus-enhancing stacks on top of an already-stressed HPA axis get modest results at best. The acute performance tools work fine on a well-regulated system. On a chronically cortisol-elevated system, you are fighting biology. Ashwagandha addresses that problem at the source.
The Mechanisms: How Ashwagandha Works
Primary Mechanism: HPA Axis Regulation
The hypothalamic-pituitary-adrenal (HPA) axis is the body’s central stress response system. When you perceive a threat — physical, psychological, or physiological — the hypothalamus signals the pituitary, which signals the adrenals to release cortisol. In the short term, this is adaptive. Cortisol mobilizes energy and sharpens alertness. In the long term, chronically elevated cortisol actively damages cognitive function: it impairs hippocampal neurogenesis, degrades working memory capacity, disrupts sleep architecture, and increases anxiety — all compounding over time.
Ashwagandha’s primary mechanism is HPA axis modulation. Its active compounds — primarily withanolides (steroidal lactones), sitoindosides, and alkaloids — appear to regulate the HPA axis feedback loop, reducing the magnitude of cortisol release in response to stressors. This is measurable across multiple RCTs through serum and salivary cortisol assays. Critically, this is not sedation or blunting — it is normalization. Ashwagandha does not prevent appropriate cortisol release in genuinely acute situations. It reduces the chronic baseline elevation that characterizes modern psychological stress.
Cholinergic Pathway and Neuroplasticity
Beyond the HPA axis, Ashwagandha appears to have direct effects on the cholinergic system relevant to memory and learning. Withanolides have demonstrated acetylcholinesterase-inhibiting properties in preclinical models — acetylcholinesterase is the enzyme that breaks down acetylcholine, so inhibiting it preserves acetylcholine availability in synaptic clefts, supporting memory formation and consolidation. This mechanism is the same pathway targeted by pharmaceutical drugs for Alzheimer’s disease (donepezil, galantamine), though Ashwagandha’s effects are substantially milder and indirect. Ashwagandha also promotes synaptic plasticity and has demonstrated neuroprotective effects in preclinical models, supporting long-term brain health and structural resilience.
GABAergic Modulation and Sleep Quality
The species name somnifera — Latin for “sleep-inducing” — hints at Ashwagandha’s well-documented effects on sleep quality. Its triethylene glycol component has demonstrated sleep-promoting properties, likely through GABA-A receptor modulation. In human RCTs, Ashwagandha consistently improves sleep onset latency, sleep quality scores, and specifically slow-wave (deep) sleep duration. This matters enormously for cognitive performance because the majority of memory consolidation, synaptic pruning, and metabolic waste clearance occurs during deep sleep. Improving sleep architecture is one of the highest-leverage interventions in any cognitive protocol — and one of the most underappreciated benefits of this compound.
What the Research Actually Shows
Ashwagandha has a larger clinical trial base than most adaptogens. I’ll walk through the key studies by outcome category because the pattern of evidence across the literature matters more than any single result.
Stress and Cortisol Reduction
Benchmark RCT — Stress & Cortisol
Chandrasekhar et al. (2012) — The KSM-66 Cortisol Study
The most cited Ashwagandha study: randomized, double-blind, placebo-controlled in 64 adults with a history of chronic stress. Participants received 300mg KSM-66 twice daily (600mg total) or placebo for 60 days. Results: serum cortisol reduced by 27.9% in the Ashwagandha group versus a small increase in placebo. Perceived Stress Scale scores, General Health Questionnaire scores, and Depression Anxiety Stress Scale scores all reached significance. This study measures objective biomarkers — not just self-report — making it methodologically stronger than much of the adaptogen literature.
Chandrasekhar K, et al. Indian J Psychol Med. 2012;34(3):255-262
Meta-Analysis — 12 RCTs
Akhgarjand et al. (2022) — Systematic Review of Stress and Anxiety
This meta-analysis synthesized 12 RCTs covering 1,002 total participants. Ashwagandha supplementation significantly reduced anxiety (SMD: −1.55) and stress (SMD: −1.75) versus placebo. Optimal dosing at 300–600mg/day confirmed in dose-response analysis. Important limitation acknowledged by the authors: certainty of evidence was rated “low” due to heterogeneity across study populations — a genuine caveat worth noting before assuming uniform effect sizes.
Cognitive Performance
Memory & Cognition RCT
Choudhary et al. (2017) — Memory and Cognitive Function
Randomized, double-blind, placebo-controlled in 50 adults with mild cognitive impairment. 300mg KSM-66 twice daily for 8 weeks. Using Wechsler Memory Scale, the Ashwagandha group showed significant improvements in immediate memory, general memory, executive function, attention, and information processing speed. The MCI population is meaningful here — these are people with genuine measurable cognitive deficits, not merely stressed healthy adults. Effects in that population suggest real cognitive impact beyond just stress reduction.
Healthy Stressed Adults — CANTAB Battery
Gopukumar et al. (2021) — The Most Relevant Study for This Audience
130 healthy stressed adults (PSS score 14–24, ages 20–55) randomized to 300mg Ashwagandha SR or placebo for 90 days. Assessment used the Cambridge Neuropsychological Test Automated Battery — the same platform I recommend for personal cognitive tracking. Results: significantly improved recall memory, lower pattern recall error rates, reduced PSS scores, reduced cortisol, improved sleep quality scores, and improved psychological well-being. This is the closest study design to the NeuroEdge audience: professionals under meaningful stress wanting to maintain and enhance cognitive performance.
Gopukumar K, et al. Evid Based Complement Alternat Med. 2021;2021:8254344
The honest summary: the strongest and most consistent cognitive effects are seen in populations with elevated stress and measurable stress-related cognitive impairment. Effects in low-stress healthy individuals are less consistent. The 2019 systematic review by Ng et al. concluded that Ashwagandha “improved performance on cognitive tasks, executive function, attention, and reaction time” across most instances, while noting heterogeneous study populations. The NIH Office of Dietary Supplements fact sheet provides the most thorough independent summary of the evidence base.
Dosing: Standardized Extracts, Forms, and What I Use Personally
Before discussing doses, the form distinction matters significantly. Ashwagandha products range from whole root powder to standardized branded extracts with verified withanolide content. The research that matters uses standardized forms — primarily KSM-66 and Sensoril — and that research is not necessarily transferable to generic root powder products of uncertain active compound content.
⬇ Free Download
Get the 7-Day Brain Optimization Protocol
The evidence-based behavioral and supplement framework for your first week of cognitive enhancement — covering sleep optimization, L-theanine + caffeine, creatine, Lion’s Mane, and the daily protocols that make them work. Completely free.
Join 2,000+ readers optimizing their cognitive performance. No spam, ever. Unsubscribe anytime.
Timing and Onset: The Most Important Expectation to Set
Ashwagandha is not an acute nootropic. You will not feel it within an hour. Most people notice nothing for the first 1–2 weeks, and this is normal. The research consistently shows effects emerging at 4 weeks and reaching full expression at 8–12 weeks of consistent daily use. Anyone who stops at week 3 because they “don’t feel anything” has made the most common Ashwagandha mistake. HPA axis recalibration is a slow physiological process — not a receptor-level interaction that produces same-day effects.
What the onset experience actually looks like: most people first notice improved sleep quality in weeks 2–3. Reduced reactivity to stressors — feeling less “triggered” by things that normally spike stress — typically emerges in weeks 3–5. Cognitive improvements are usually last, often at weeks 6–8, and are most noticeable as improved memory recall, better sustained concentration, and reduced mental fatigue during demanding work.
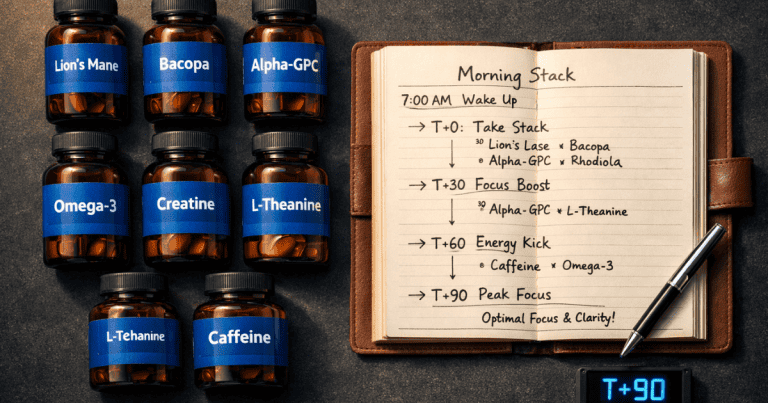
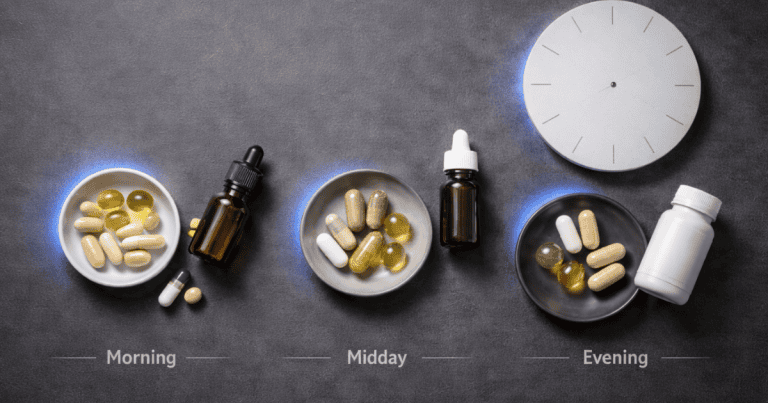
Practical Timing Framework
300mg KSM-66 with breakfast. Food reduces GI upset. Morning dose supports daytime cortisol regulation and stress resilience.
300mg KSM-66 with dinner or 60–90 min before bed. Evening dose leverages the sleep quality benefit. Some users find this mildly sedating — usually a feature, not a problem.
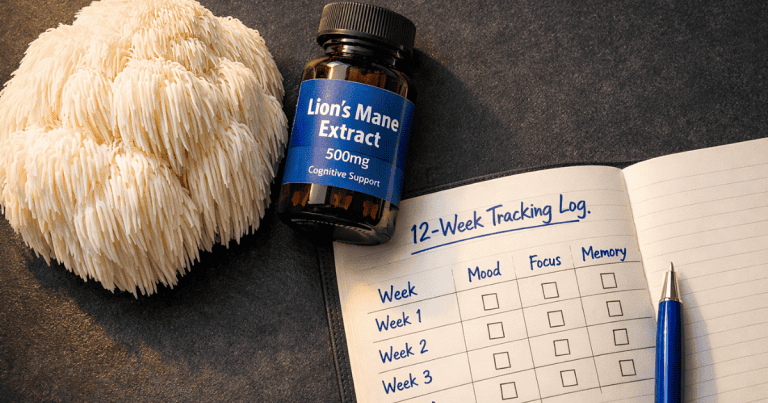
No noticeable effect is normal. Consistent daily use is the protocol. Do not evaluate whether it’s “working” during this period.
Stress reactivity and sleep quality improving. Begin tracking with PSS-10 questionnaire and Cambridge Brain Sciences cognitive battery.
Full assessment point. Compare scores against baseline. Consider a 2–4 week break to re-establish baseline, then assess the difference on return to confirm continued contribution.
Sourcing: Why the Form on the Label Matters
Both KSM-66 and Sensoril are legitimate, research-backed forms with documented production standards. For cognitive enhancement and stress resilience as the primary goals, KSM-66 is the default recommendation because it has the deepest cognitive research base. For sleep quality as the primary goal, Sensoril is a reasonable alternative. The choice matters less than using a verified standardized form rather than a generic root powder product with undefined withanolide content.
Independent testing by ConsumerLab has identified significant variability in Ashwagandha products, including products with substantially less active compound than labeled. For a compound where the safety data includes liver toxicity cases, using a product with verified third-party testing and a Certificate of Analysis is the minimum acceptable standard. The specific branded extract — KSM-66 or Sensoril — should be named on the label, not just “Ashwagandha root extract.” Branded ingredients indicate standardized production with verified withanolide percentage.
Safety, Contraindications, and Who Should Not Use Ashwagandha
Ashwagandha has a more complex safety profile than its mainstream popularity implies. The clinical trial data is generally favorable — in studies up to 3 months, adverse effects were typically mild GI complaints (loose stools, nausea, drowsiness). But there are three areas requiring explicit, honest discussion: liver toxicity, thyroid effects, and autoimmune conditions.
Liver Toxicity: Real, Rare, and Worth Taking Seriously
Cases of Ashwagandha-induced liver injury have been documented from Japan, Iceland, India, and the US. The typical pattern is cholestatic hepatitis appearing 2–12 weeks after starting use, presenting as jaundice, pruritus, and elevated liver enzymes. In most cases, the condition resolves on discontinuation. In rare cases — primarily in individuals with pre-existing liver disease — severe outcomes including liver failure have been reported. The proposed mechanism involves withanone forming DNA adducts when glutathione detoxification capacity is overwhelmed, classified as an idiosyncratic response. It cannot be predicted from dose alone and does not occur commonly at recommended doses. But it is documented across multiple countries and healthcare systems, and it demands honest acknowledgment. Anyone with pre-existing liver disease should not use Ashwagandha.
Thyroid Effects: Beneficial for Some, Dangerous for Others
Ashwagandha has demonstrated the ability to increase thyroid hormone levels (T3 and T4). A 2017 RCT found that 600mg/day normalized thyroid indices in subclinical hypothyroid patients over 8 weeks — for that population, the thyroid effect is a feature. For anyone with hyperthyroidism, Hashimoto’s thyroiditis, Graves’ disease, or who takes thyroid hormone medications, this same effect represents a meaningful risk. The NCCIH explicitly recommends against Ashwagandha use in people with thyroid disorders. This is one of the clearer contraindications in the supplement literature.
Autoimmune Conditions
Ashwagandha’s immunostimulatory properties are beneficial for most people but potentially problematic for individuals with autoimmune conditions — multiple sclerosis, lupus, rheumatoid arthritis, inflammatory bowel disease — where further immune activation may worsen symptoms. If you have a diagnosed autoimmune condition, this is a conversation for your healthcare provider, not a supplement decision to make independently.
Avoid Ashwagandha if you have:
Pre-existing liver disease or elevated liver enzymes · Hyperthyroidism or Graves’ disease · Hashimoto’s thyroiditis or autoimmune thyroid conditions · Any diagnosed autoimmune condition · Scheduled surgery within 2 weeks · Pregnancy (avoid entirely) · Hormone-sensitive prostate cancer
Discuss with your healthcare provider if you take:
Thyroid hormone medications · Antidiabetic medications (blood glucose lowering risk) · Antihypertensive medications (additive blood pressure lowering) · Immunosuppressants · Sedatives or CNS depressants
Where Ashwagandha Fits in a Complete Cognitive Protocol
The framing I use: Ashwagandha is a foundation compound, not a performance compound. The L-theanine + caffeine stack provides acute focus enhancement for specific high-demand windows. Ashwagandha provides the system-level stability that makes those acute performance tools work consistently. A well-regulated HPA axis means your cognitive capacity is operating near its actual ceiling rather than at 70% because chronic stress is consuming the resources.
The clearest indicators that Ashwagandha belongs in your protocol: you experience meaningful chronic psychological stress, your sleep quality is inconsistent, you notice your cognitive performance varying significantly with your stress load, and you’ve already built the behavioral foundations covered in the Focus & Productivity framework. If you haven’t done the behavioral work, Ashwagandha alone will help but you are treating symptoms rather than root causes.
The clearest indicator it doesn’t belong in your current protocol: low baseline stress, consistently high-quality sleep, and cognitive performance that doesn’t fluctuate meaningfully with stress load. In that case, the marginal benefit of HPA axis modulation is small and the safety considerations make it not worth adding. Use it when the problem it solves is actually present in your system.
Frequently Asked Questions
How long does Ashwagandha take to work?
Most people notice improved sleep quality in weeks 2–3 as the first sign. Reduced stress reactivity typically emerges in weeks 3–5. Measurable cognitive improvements — better memory recall, improved attention, reduced mental fatigue — usually appear at 6–8 weeks of consistent daily use. Full effects are typically established by week 12. Stopping at week 3 because you feel nothing is the most common mistake with this compound. The mechanism is HPA axis recalibration — a slow physiological process, not a same-day effect.
Should I take Ashwagandha in the morning or at night?
Both, ideally. The research-supported protocol is 300mg twice daily — morning with breakfast and evening with dinner or 60–90 minutes before bed. The morning dose supports daytime stress regulation; the evening dose leverages the sleep quality benefit. If only dosing once daily, the evening dose has a slight edge because improved sleep architecture is usually the most noticeable early benefit. Take with food to reduce GI upset.
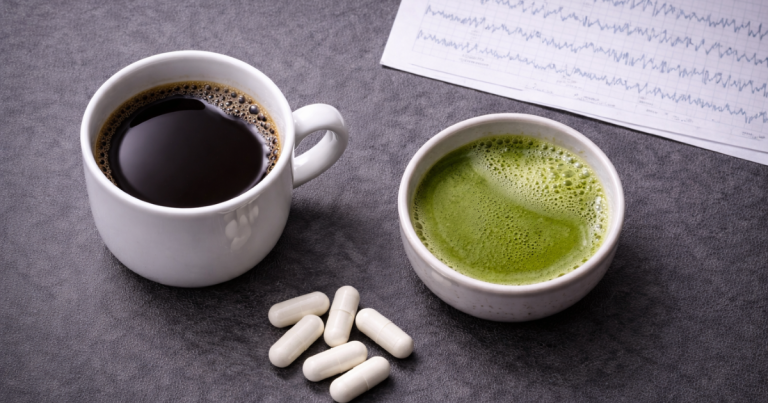
Can I take Ashwagandha with my L-theanine and caffeine stack?
Yes. They operate through entirely different mechanisms and target different aspects of cognitive performance. Ashwagandha is foundational infrastructure — HPA axis regulation, sleep quality, chronic stress reduction. L-theanine + caffeine is acute performance enhancement for specific high-demand windows. No known adverse interactions exist. The combination is actually a natural pairing: Ashwagandha addresses the chronic system-level stress that degrades cognitive baseline; the L-theanine + caffeine stack performs within that improved baseline.
Does Ashwagandha need to be cycled?
The evidence does not suggest tolerance development the way stimulant-based compounds require cycling. The HPA axis mechanism does not undergo the receptor downregulation seen with adenosine receptors and caffeine. I personally take 2–4 week breaks every 3–4 months primarily to re-establish baseline and confirm continued contribution, not because tolerance is a documented concern. Long-term safety beyond 3 months is less well-studied — a genuine limitation worth acknowledging in any honest discussion of this compound.
Is KSM-66 worth the price premium over generic Ashwagandha?
For cognitive enhancement purposes, yes — not because the branded form has uniquely superior properties, but because the research is conducted on KSM-66 specifically. Using it means the dose you take corresponds to the dose that produced the documented effects. Generic root powder varies substantially in active withanolide content by harvest, source, and processing. Given that you’ll be taking it consistently for 12+ weeks waiting for the full effect to develop, starting with the verified form is worth the modest price premium.
Scientific References
- Chandrasekhar K, Kapoor J, Anishetty S. “A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of Ashwagandha root in reducing stress and anxiety in adults.” Indian J Psychol Med. 2012;34(3):255-262. pubmed.ncbi.nlm.nih.gov/23439798
- Choudhary D, Bhattacharyya S, Bose S. “Efficacy and Safety of Ashwagandha Root Extract in Improving Memory and Cognitive Functions.” J Diet Suppl. 2017;14(6):599-612. pubmed.ncbi.nlm.nih.gov/28471731
- Gopukumar K, et al. “Efficacy and Safety of Ashwagandha Root Extract on Cognitive Functions in Healthy, Stressed Adults.” Evid Based Complement Alternat Med. 2021;2021:8254344. pubmed.ncbi.nlm.nih.gov/34858513
- Akhgarjand C, et al. “Does Ashwagandha supplementation have a beneficial effect on the management of anxiety and stress? A systematic review and meta-analysis.” Phytother Res. 2022;36(11):4115-4124. pubmed.ncbi.nlm.nih.gov/36017529
- Lopresti AL, et al. “An investigation into the stress-relieving and pharmacological actions of an ashwagandha extract.” Medicine (Baltim). 2019;98(37):e17186. pubmed.ncbi.nlm.nih.gov/31517876
- Ng QX, et al. “A systematic review of the clinical use of Withania somnifera (Ashwagandha) to ameliorate cognitive dysfunction.” Phytother Res. 2020;34(3):583-590. pubmed.ncbi.nlm.nih.gov/31742775
- NIH Office of Dietary Supplements. “Ashwagandha: Health Professional Fact Sheet.” Updated 2025. ods.od.nih.gov/factsheets/Ashwagandha-HealthProfessional
- National Center for Complementary and Integrative Health. “Ashwagandha: Usefulness and Safety.” nccih.nih.gov/health/ashwagandha
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. “Ashwagandha.” NIDDK. ncbi.nlm.nih.gov/books/NBK548536
- Sharma AK, et al. “Efficacy and Safety of Ashwagandha Root Extract in Subclinical Hypothyroid Patients.” J Altern Complement Med. 2018;24(3):243-248. pubmed.ncbi.nlm.nih.gov/28829155