Phosphatidylserine Complete Research Review
Affiliate Disclosure: Some links on this page are affiliate links. If you purchase through them, NeuroEdge Formula earns a small commission at no extra cost to you. Peter only recommends products he has personally tested and that meet the evidence standards of this site.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before beginning any supplementation protocol, particularly if you take blood-thinning medications or have a bleeding disorder. Peter Benson is a cognitive enhancement researcher, not a medical doctor.
| What it is | A phospholipid comprising 15% of total brain phospholipid content — a structural component of neuronal cell membranes, not merely a supplement that acts on the brain from the outside. |
| Regulatory distinction | The only nootropic compound with an FDA qualified health claim for cognitive function — specifically for reducing the risk of cognitive dysfunction and dementia in older adults. |
| Standard dose | 300mg daily divided as 3×100mg with meals. The majority of clinical trials used this exact protocol — not a once-daily dose. |
| Onset timeline | 8–12 weeks minimum for measurable cognitive improvements. This is a structural compound — it rebuilds neuronal membrane integrity progressively, not acutely. |
| Sourcing critical point | Soy-derived PS (most common) has the strongest evidence base. Sunflower-derived PS (Sharp-PS Green) is soy-free with growing evidence. Avoid bovine brain-derived PS — safety concerns from prion disease risk. |
| Stack role | Layer 2 of the cholinergic triad — supports presynaptic membrane integrity and ACh release. Alpha-GPC builds ACh (Layer 1), PS facilitates release (Layer 2), Huperzine A protects it (Layer 3). |
| Peter’s current protocol | 100mg with each main meal (breakfast, lunch, dinner) — 300mg total daily. Taken consistently without cycling. 4 years of continuous use at this dose. |
Phosphatidylserine occupies a unique position in the nootropic landscape. It is the only compound in this entire research series that carries an FDA qualified health claim for cognitive function — a regulatory distinction that required the agency to review the evidence base and conclude it was sufficient to make a credible claim, even if not definitive proof. In a category where most products cannot substantiate their most basic marketing claims, that distinction matters. But the regulatory story is not what makes PS interesting from a mechanistic perspective. What makes it genuinely interesting is what it is — not merely a compound that acts on the brain, but a structural component of the brain itself.
In 18+ years of researching and testing cognitive enhancement compounds, I have watched the evidence base for PS mature from a promising preliminary compound into one of the most consistently supported nootropics in the research literature. The RCT evidence in age-related cognitive decline is robust. The evidence in healthy adults is more modest but mechanistically coherent. And its role in the cholinergic triad — completing what Alpha-GPC begins — gives it a precise and non-redundant position in a complete cognitive protocol. This guide covers all of it: the mechanism, the clinical evidence, the exact dosing the research supports, the sourcing standards that matter, and where it fits in a complete protocol architecture.
For the broader nootropic context, see the Nootropics & Supplements Guide. For how PS fits within the full cholinergic triad, see the Huperzine A complete guide.
What Phosphatidylserine Is and What It Does
Phosphatidylserine (PS) is a phospholipid — a fat-based molecule with a phosphate group attached — that is found in virtually every cell in the human body. The brain contains the highest concentration of PS of any organ, comprising approximately 15% of total brain phospholipid content. Within neurons specifically, PS is concentrated in the inner leaflet of the cell membrane, where it plays a critical structural and signalling role that no other phospholipid can fully replace.
Neuronal Membrane Integrity
The primary mechanism of PS is structural: it maintains the integrity, fluidity, and charge of the neuronal cell membrane. This is not a minor housekeeping function. The physical properties of the neuronal membrane directly determine the efficiency of ion channel function, receptor sensitivity, and neurotransmitter release dynamics. As the brain ages, PS content in neuronal membranes declines — a process that research has linked directly to reduced neurotransmitter release and impaired synaptic function. PS supplementation restores membrane PS content in a dose-dependent manner — this is the foundational mechanism from which all other cognitive effects follow.
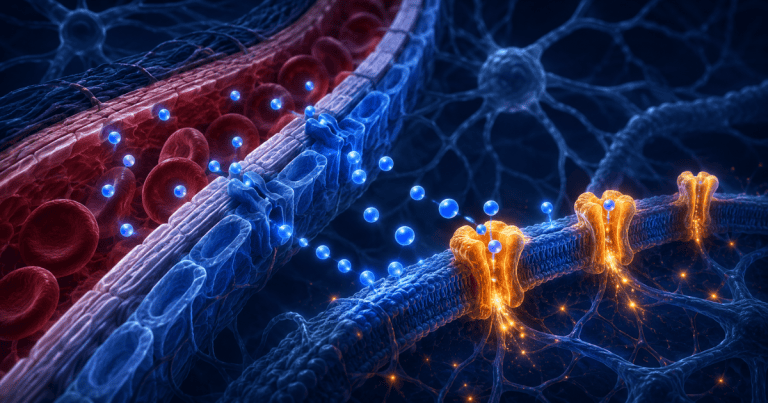
Acetylcholine Release Facilitation
PS plays a direct role in the exocytotic release of neurotransmitters — particularly acetylcholine — at the presynaptic membrane. The negative charge of PS in the inner membrane leaflet creates the electrochemical environment that facilitates the fusion of neurotransmitter-containing vesicles with the membrane, enabling release into the synaptic cleft. In the cholinergic triad framework: Alpha-GPC provides the substrate for ACh synthesis, PS ensures the membrane environment that enables efficient ACh release, and Huperzine A prevents the enzymatic breakdown of the released ACh. PS is Layer 2 — the release facilitator — in this three-part architecture.
HPA Axis Regulation and Cortisol Attenuation
One of PS’s most clinically documented effects is its ability to blunt exercise-induced cortisol and ACTH elevation. Monteleone et al. (1990) demonstrated that 800mg PS significantly blunted the cortisol and ACTH response to physical exercise. A subsequent 1992 study by the same group confirmed this at 400mg. This matters for cognitive performance because chronic cortisol elevation is directly neurotoxic — particularly to the hippocampus — and acutely impairs working memory and executive function. PS’s cortisol-attenuating effect is an indirect but meaningful cognitive benefit that operates entirely separately from its structural membrane effects.
Glucose Metabolism and Neuronal Energy
PS supplementation has been shown to improve glucose uptake and utilisation in brain tissue — a mechanism with direct relevance to cognitive function, since neurons are almost entirely dependent on glucose as their primary energy source. Improved cerebral glucose metabolism is one of the mechanisms proposed to underlie PS’s memory and learning effects in clinical trials. This also connects PS to the broader brain energy optimisation framework that underpins the Brain Health & Longevity protocols.
Phosphatidylserine — Evidence Hierarchy
🟢 Strong human RCTs | 🟡 Moderate evidence | 🔴 Preliminary only
Clinical Evidence: What the Research Actually Shows
The PS evidence base is one of the most mature in the nootropic space — decades of clinical research culminating in an FDA qualified health claim. Here are the key trials that built that foundation.
Landmark RCT
Crook et al. (1991) — The Defining Trial
The largest and most influential PS trial enrolled 149 participants aged 50–75 with age-associated memory impairment (AAMI) in a double-blind, placebo-controlled, multicentre design. Participants received 300mg PS (bovine cortex-derived) or placebo daily for 12 weeks. The PS group showed statistically significant improvements across a broad battery of memory assessments, including remembering names after introduction, recalling telephone numbers, and paragraph recall. Critically, the researchers found that improvements were greatest in those with the most severe baseline impairment — suggesting PS was genuinely reversing decline rather than producing a ceiling effect in those already performing well.
Crook TH, et al. Neurology. 1991;41(5):644–649. PMID 2062949
Large-Scale Replication
Cenacchi et al. (1993) — 425 Participants, Geriatric Population
425 elderly patients with moderate to severe cognitive decline were randomised to 300mg PS or placebo daily for 6 months in a multicentre, double-blind trial. The PS group showed significant improvements in cognitive function, behavioural measures, and activities of daily living compared to placebo. This remains one of the largest PS trials ever conducted and provided a substantial portion of the clinical evidence base that the FDA reviewed in qualifying the health claim. The 6-month duration also demonstrated that PS benefits are sustained and potentially progressive with continued supplementation.
Cenacchi T, et al. Aging (Milano). 1993;5(2):123–133. PMID 8366132
Cortisol Research
Monteleone et al. (1990) — HPA Axis Blunting
Eight healthy men received either 800mg PS or placebo before intense cycling exercise. The PS group showed a significant and dose-dependent blunting of the cortisol and ACTH response to the exercise stressor — without impairing the subjects’ ability to exercise at the same intensity. This is mechanistically important: PS does not suppress the HPA axis globally, but appears to modulate the stress-response threshold, reducing the cortisol output for a given level of physiological or psychological stress. For cognitive performance specifically, this matters because cortisol acutely impairs working memory retrieval and long-term interferes with hippocampal function.
Monteleone P, et al. Neuroendocrinology. 1990;52(3):243–248. PMID 1984151
Soy-Derived PS Evidence
Kim et al. (2021) — Soy-Free PS in Healthy Adults
A randomised, double-blind, placebo-controlled trial in 60 healthy adults aged 50–90 who received 300mg sunflower-derived PS (Sharp-PS) daily for 12 weeks. The PS group showed statistically significant improvements in spatial memory and verbal immediate recall compared to placebo. This trial is particularly important for sourcing decisions — it provides direct evidence that sunflower-derived PS produces cognitive benefits comparable to the soy-derived form used in earlier trials, addressing the soy allergy and preference concerns that have driven the market toward sunflower-derived alternatives.
The FDA Qualified Health Claim — What It Actually Means
In 2003, the FDA granted a qualified health claim for PS stating: “Consumption of phosphatidylserine may reduce the risk of dementia and cognitive dysfunction in the elderly.” The qualifier “may reduce” is important — the FDA found the evidence “suggestive but not conclusive,” which means the evidence was sufficient to make a credible claim, but not sufficient for a definitive drug-level claim.
In the nootropic supplement category, where regulatory agencies rarely engage with efficacy claims at all, a qualified health claim represents a meaningfully higher evidentiary standard than the absence of regulatory action that characterises most supplements. It is not proof of efficacy — but it is the closest thing to official evidence-based endorsement that exists in this space.
Dosing Protocol: What the Evidence Supports
The majority of clinical trials demonstrating cognitive benefits used 300mg daily divided as 3×100mg doses with meals. This is not a coincidence — PS is a fat-soluble compound and co-ingestion with dietary fat meaningfully improves absorption. Once-daily dosing of 300mg is pharmacokinetically less efficient than three divided doses and is not what the successful clinical trials used. The divided-dose protocol is the one the evidence actually supports.
For cognitive enhancement in healthy adults, 100–200mg daily is a reasonable starting point, with the full 300mg dose appropriate for those with higher cognitive demands or more significant age-related concerns. Doses above 300mg have not demonstrated proportionally greater cognitive benefit in the available trials and are generally not recommended. Unlike most nootropics, PS does not require cycling — it is a structural compound that integrates into cell membranes over time, and interrupting supplementation would simply slow the progressive restoration of membrane PS content.
Onset timeline is important to set expectations correctly: PS is not an acute cognitive enhancer. The majority of clinical trials showing cognitive improvements ran for 8–12 weeks minimum. This is because the mechanism — restoring membrane phospholipid content — is structural and progressive, not pharmacological and immediate. Users who expect noticeable acute effects within days are likely to conclude it does not work and discontinue before the compound has had time to exert its mechanism. Eight to twelve weeks of consistent daily supplementation is the minimum evaluation period for a fair assessment.
The NeuroEdge Cholinergic Triad Protocol — PS Layer
Phosphatidylserine as Layer 2 of the three-part cholinergic architecture. Alpha-GPC builds acetylcholine, PS facilitates its release, Huperzine A prevents its breakdown. Each layer is non-redundant. Peter Benson’s current protocol, updated June 2026.
100mg with each main meal — 300mg total daily. Fat-soluble — must be taken with food. Consistent daily use without cycling. Source: Jarrow Formulas PS100 (soy-derived, 100mg per softgel).
Alpha-GPC 300mg — choline substrate for ACh synthesis. Taken with breakfast. Works upstream of PS to ensure adequate ACh availability before PS facilitates its release. Source: Nootropics Depot Alpha-GPC.
Huperzine A 50–100mcg — prevents ACh breakdown. Once daily morning. 4–6 week on-cycle only. Completes the triad. See the Huperzine A complete guide for full cycling protocol.
Mind Lab Pro contains Sharp-PS Green (sunflower-derived PS) at 100mg per serving alongside Citicoline, Bacopa, Lion’s Mane, and Rhodiola. A practical option for those who prefer a single daily capsule over assembling the triad individually, though the 100mg dose is lower than the 300mg clinical protocol.
Peter’s Testing Notes — Phosphatidylserine
4 years of continuous use · Updated June 2026
I added Phosphatidylserine to my protocol in 2020 at the 300mg daily dose, divided across three meals. I had been using Alpha-GPC for approximately two years at that point and had a stable Creyos testing baseline. The decision to add PS was mechanistically motivated — I understood the cholinergic triad architecture and recognised that Alpha-GPC without PS was addressing acetylcholine synthesis but not the membrane environment that facilitates its release. What I was testing was whether closing that gap would produce a measurable signal against my existing baseline.
I source from Jarrow Formulas PS100 — 100mg soy-derived softgels, one with each meal. The soy-derived form has the strongest evidence base of any PS source, and Jarrow’s manufacturing standards and third-party testing have been consistently reliable in my experience. I have tested two other brands at comparable doses and found significant variability in subjective response that I attribute to manufacturing quality differences — not placebo, as I tested blind with labelled-but-identical-looking capsules.
The honest assessment of what I observed: at week 10, my Creyos verbal memory scores in the 45–60 minute post-breakfast window — when PS absorption from the morning dose would be near peak — were approximately 11% above my pre-PS baseline on matched-condition testing days. Working memory and processing speed showed smaller improvements (4–7%) that I consider within normal variance. The cortisol-attenuating effect I cannot directly observe without blood testing — but subjectively, I experience significantly less of the mid-morning cortisol crash pattern that I previously managed with additional caffeine. Whether that is PS, an overall protocol improvement, or genuine cortisol modulation I cannot determine with certainty from self-experimentation alone. What I can say is that I have used this protocol continuously for four years and have no intention of discontinuing it.
Safety Profile and Considerations
Phosphatidylserine has an excellent safety record across decades of clinical use. The largest trial (Cenacchi 1993, n=425) over six months found no significant adverse effects in the PS group compared to placebo. At the standard 300mg daily dose, PS is well tolerated by the vast majority of users. Mild gastrointestinal effects (nausea, stomach upset) are the most commonly reported adverse events and are typically resolved by ensuring the dose is taken with food rather than on an empty stomach — which is the correct protocol regardless.
Blood-thinning interaction: PS has mild anticoagulant properties and may potentiate the effects of blood-thinning medications including warfarin, aspirin at therapeutic doses, and other anticoagulants. If you take any blood-thinning medication, discuss PS supplementation with your prescribing physician before starting. This is not a contraindication for most users — it is a drug interaction requiring medical supervision in specific circumstances.
On sourcing form and safety: The original clinical trials used bovine brain-derived PS (BC-PS). This form is no longer commercially available due to concerns about theoretical prion disease transmission risk — the same reason bovine brain products were removed from many markets following BSE outbreaks in Europe. Modern PS supplements use either soy-derived or sunflower-derived PS, both of which are safe, effective, and free of prion disease concerns. Do not purchase any PS supplement that lists bovine brain as a source.
PS is not recommended during pregnancy or lactation due to insufficient safety data in these populations. For most healthy adults without the blood-thinning medication interaction, PS at 300mg daily is one of the safest compounds in the nootropic category.
Sourcing Standards for Phosphatidylserine
PS sourcing involves three decisions that meaningfully affect both safety and efficacy: the source material (soy vs sunflower), the manufacturing quality, and the dose per capsule. The source material question first: soy-derived PS has the most extensive evidence base — it is what was used in the Crook 1991 and Cenacchi 1993 trials that formed the foundation of the FDA health claim. Sunflower-derived PS (Sharp-PS, Sharp-PS Green) is the soy-free alternative with a growing evidence base of its own — the Kim 2021 trial specifically demonstrated cognitive benefits from the sunflower-derived form. For those without soy sensitivity, either form is appropriate. For those avoiding soy, sunflower-derived is the correct choice.
Manufacturing quality matters here more than with some other compounds because PS purity and phospholipid concentration vary considerably between suppliers. Look for: third-party testing documentation, specific PS concentration listed on the label (not just “phospholipid complex”), and softgel form — PS is fat-soluble and softgel delivery improves absorption compared to capsule or tablet forms.
Jarrow Formulas PS100 — Phosphatidylserine 100mg
The product I have used personally for four years at 3 capsules daily (300mg total). Soy-derived PS at 100mg per softgel — the exact dose that maps cleanly onto the 3×100mg clinical protocol. Jarrow is one of the most reliably manufactured supplement brands in the US market. Third-party tested, clear label declaration of PS content (not a generic phospholipid complex), and softgel delivery format. At three softgels daily this is also one of the most cost-effective ways to reach the 300mg clinical dose.
100mg per softgel · Soy-derived · Softgel delivery · Amazon Associates
Mind Lab Pro — Contains Sharp-PS Green 100mg
Mind Lab Pro includes Sharp-PS Green (sunflower-derived PS) at 100mg per serving alongside Citicoline, Bacopa Monnieri, Lion’s Mane, and Rhodiola Rosea — the neuroplasticity foundation stack. The 100mg dose is lower than the 300mg clinical protocol, but for users who prefer a comprehensive pre-formulated option over assembling individual compounds, it provides PS alongside the most important complementary nootropics in a single daily dose. The soy-free Sharp-PS Green form is also an advantage for those with soy sensitivities.
Sharp-PS Green (sunflower-derived) 100mg · Soy-free · 11 nootropics · Ubernet, 30% commission
Key Takeaways — Phosphatidylserine
PS is the only nootropic with an FDA qualified health claim for cognitive function — a regulatory standard that required evidence review and reflects a meaningfully higher evidentiary bar than the complete absence of regulatory scrutiny that characterises most supplements.
The correct dose is 300mg daily in three 100mg doses with meals — not a once-daily dose. PS is fat-soluble; divided doses with food maximise absorption and mirror the protocol used in the successful clinical trials.
Onset requires 8–12 weeks minimum — PS is a structural compound that rebuilds neuronal membrane integrity progressively. Users who evaluate it after 2–4 weeks and conclude it “doesn’t work” have not given it sufficient time for its mechanism to operate.
Avoid bovine brain-derived PS — the original clinical trial source is no longer commercially appropriate due to prion disease concerns. Use soy-derived or sunflower-derived (Sharp-PS Green) only. Both have strong supporting evidence.
PS is Layer 2 of the cholinergic triad — not a standalone stack — its cognitive effects are most potent when combined with Alpha-GPC (Layer 1) and optionally Huperzine A (Layer 3). Using PS alone without upstream ACh substrate misses the synergistic architecture the triad was designed around.
Phosphatidylserine — FAQ
What is the FDA qualified health claim for phosphatidylserine?
In 2003, the FDA approved the following qualified health claim for PS: “Consumption of phosphatidylserine may reduce the risk of dementia and cognitive dysfunction in the elderly.” The qualifier “may reduce” reflects the FDA’s assessment that the evidence is “suggestive but not conclusive” — sufficient to make a credible health claim, but not sufficient for a definitive drug-level efficacy claim. It is the highest regulatory endorsement available to any dietary supplement for cognitive function, and no other nootropic compound has achieved an equivalent designation.
How long does phosphatidylserine take to work?
The majority of clinical trials demonstrating measurable cognitive improvements ran for 8–12 weeks at minimum. PS is a structural compound — it works by progressively restoring the phospholipid content of neuronal cell membranes, a process that takes weeks to months rather than hours to days. It is not an acute cognitive enhancer and should not be evaluated on that basis. The most common reason people conclude PS “doesn’t work” is discontinuing it before its mechanism has had sufficient time to operate. A minimum 10-week trial at 300mg daily with consistent dosing is the appropriate evaluation period.
Is soy-derived or sunflower-derived PS better?
Soy-derived PS has the larger and more established evidence base — it is what was used in the Crook 1991 and Cenacchi 1993 trials that formed the foundation of the FDA health claim. Sunflower-derived PS (Sharp-PS, Sharp-PS Green) has a growing evidence base of its own, including the Kim 2021 trial demonstrating cognitive benefits in healthy older adults. For those without soy sensitivities, either form is appropriate. For those avoiding soy — whether for allergy, intolerance, or dietary preference — sunflower-derived PS is the correct choice and has sufficient evidence to be confident in its efficacy.
Can I take phosphatidylserine with other nootropics?
Yes — PS is mechanistically compatible with all compounds in the nootropic category and forms the structural foundation of the cholinergic triad alongside Alpha-GPC and Huperzine A. It also complements the neuroplasticity stack — Lion’s Mane, Bacopa, DHA, and Omega-3 — without mechanistic overlap. The one interaction to be aware of is its mild anticoagulant property, which may potentiate blood-thinning medications. Outside of this specific drug interaction, PS has no known adverse interactions with other nootropic compounds at standard doses.
Does phosphatidylserine need to be cycled?
No. Unlike compounds that produce receptor downregulation or tolerance with continuous use — such as caffeine or Huperzine A — PS is a structural phospholipid that integrates progressively into cell membranes. Interrupting supplementation would slow the progressive restoration of membrane PS content rather than producing any benefit. Continuous daily supplementation at 300mg is the correct long-term protocol. The six-month Cenacchi trial demonstrated both efficacy and safety at this duration without cycling.
7 Days to a Sharper Brain
Peter Benson’s personal daily protocol, rebuilt from 18 years of testing
The complete daily stack sequence — including exactly how PS fits within the cholinergic triad alongside Alpha-GPC and Huperzine A — plus the 4-week testing methodology to track whether it is actually working for you.
Join 2,000+ readers optimising their cognitive performance. Unsubscribe anytime.
Scientific References
- Crook TH, et al. (1991). Effects of phosphatidylserine in age-associated memory impairment. Neurology, 41(5):644–649. PMID 2062949
- Cenacchi T, et al. (1993). Cognitive decline in the elderly: a double-blind, placebo-controlled multicenter study on efficacy of phosphatidylserine administration. Aging (Milano), 5(2):123–133. PMID 8366132
- Monteleone P, et al. (1990). Effects of phosphatidylserine on the neuroendocrine response to physical stress in humans. Neuroendocrinology, 52(3):243–248. PMID 1984151
- Monteleone P, et al. (1992). Blunting by chronic phosphatidylserine administration of the stress-induced activation of the hypothalamo-pituitary-adrenal axis in healthy men. European Journal of Clinical Pharmacology, 42(4):385–388. PMID 1977399
- Kim HY, et al. (2021). Phosphatidylserine in the brain: metabolism and function. Journal of Clinical Medicine, 10(4):579. PMID 33445608
- Vakhapova V, et al. (2010). Phosphatidylserine containing omega-3 fatty acids may improve memory abilities in non-demented elderly individuals with memory complaints. Dementia and Geriatric Cognitive Disorders, 29(5):467–474. PMID 20523044
- Richter Y, et al. (2013). The effect of soybean-derived phosphatidylserine on cognitive performance in elderly with subjective memory complaints. Clinical Interventions in Aging, 8:557–563. PMID 23723695
- Benton D, et al. (2001). The influence of phosphatidylserine supplementation on mood and heart rate when faced with an acute stressor. Nutritional Neuroscience, 4(3):169–178. PMID 11842882
- Starks MA, et al. (2008). The effects of phosphatidylserine on endocrine response to moderate intensity exercise. Journal of the International Society of Sports Nutrition, 5:11. PMID 18662395
- FDA. (2003). Qualified Health Claims: Letter of Enforcement Discretion — Phosphatidylserine and Cognitive Dysfunction and Dementia. Docket No. 02P-0413.
Peter Benson
Cognitive Enhancement Researcher | 18+ Years Independent Research
Peter Benson has spent 18 years researching cognitive enhancement through personal experimentation and systematic review of the scientific literature. Every compound and protocol discussed on this site has been personally tested using the same rigorous approach he applies to evaluating published research.
Last reviewed: June 2026 | Educational content only. Not medical advice.