Phosphatidylserine Complete Research Review
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Phosphatidylserine may interact with anticholinergic medications, anticoagulants, and blood-thinning medications. Consult a qualified healthcare provider before beginning any supplementation protocol, particularly if you take prescription medications, have a clotting disorder, or are pregnant or nursing.
Phosphatidylserine: Benefits, Dosing, and What the Research Actually Shows
The only nootropic supplement with an FDA qualified health claim for cognitive function — and a regulatory distinction that requires careful reading. What the clinical evidence actually supports, who benefits most, and why the bovine vs. soy sourcing question matters more than most guides acknowledge.
Bottom Line — For Those Who Want It First
Phosphatidylserine (PS) is the structural phospholipid that makes up 13–15% of the human cerebral cortex. It is the only dietary supplement with an FDA qualified health claim for cognitive function — though the claim comes with the FDA’s own disclaimer that evidence is “very limited and preliminary.” The honest picture: PS has consistent evidence for memory improvement in older adults with age-related memory decline and MCI, a well-characterized mechanism for cortisol blunting, and a strong safety record across decades of research. The effect size in healthy young adults is modest. It belongs in a nootropic protocol as structural brain support — particularly valuable for anyone over 40, those under significant chronic stress, or anyone using the full adaptogen + performance stack.
Standard Protocol
100–300mg soy-derived PS daily
Onset Timeline
6–12 weeks for cognitive effects
Evidence Level
FDA qualified health claim · 15+ RCTs
Best Population
Adults 40+ with memory concerns or high stress
What Phosphatidylserine Is — And Why It Is Different From Other Nootropics
Most compounds covered in the Nootropics & Supplements Guide work by modulating neurotransmitter systems, improving vascular delivery, or regulating the HPA stress axis. Phosphatidylserine works at a more fundamental level: it is a structural component of neuronal membranes themselves. Understanding this distinction is essential for using it correctly, setting realistic expectations, and explaining why it belongs in a serious long-term cognitive stack even when its acute effects are subtle.
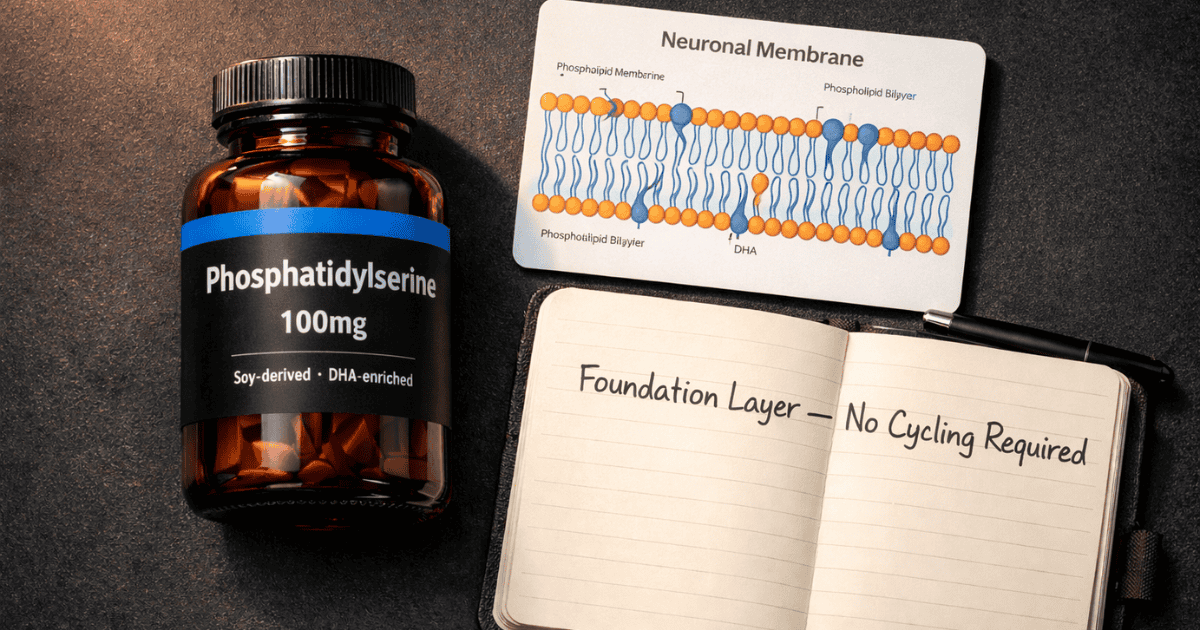
Phosphatidylserine (PS) is a glycerophospholipid — a fatty acid-based molecule that forms the lipid bilayer of cell membranes in virtually every cell in the body. In the brain specifically, PS accounts for 13–15% of the total phospholipid content of the cerebral cortex. It is concentrated almost entirely in the inner leaflet of neuronal plasma membranes, where it serves as a structural foundation for membrane-bound protein function: receptor activity, enzyme signaling, ion channel regulation, and the molecular machinery through which neurons communicate and survive. The average Western diet provides approximately 130mg of PS daily through meat, fish, and egg yolks — substantially less than the 300mg daily doses used in most clinical trials.
PS levels in the brain decline with age — a well-documented process that accelerates after 60 and correlates with the memory consolidation deficits characteristic of normal aging. This age-related PS depletion is the mechanistic foundation for the clinical evidence base: supplementation restores or maintains PS levels in neuronal membranes, supporting the structural integrity and functional capacity of cognitive circuits that are progressively depleted with age and stress. This is not the same mechanism as Ashwagandha’s HPA axis modulation or Panax ginseng’s vascular and cholinergic effects — it is structural, slower, and more foundational.
The FDA Qualified Health Claim: What It Actually Means
In May 2003, the U.S. Food and Drug Administration issued a qualified health claim for phosphatidylserine — the only such claim ever granted for a cognitive supplement. This is regularly cited in marketing material for PS products, typically without the equally important context of what a “qualified health claim” actually signifies.
The FDA’s permitted claim reads: “Consumption of phosphatidylserine may reduce the risk of dementia and cognitive dysfunction in the elderly.” The required accompanying disclaimer, which most marketing omits, reads: “Very limited and preliminary scientific research suggests that PS may reduce the risk of cognitive dysfunction in the elderly. FDA concludes that there is very little scientific evidence supporting this claim.”
A qualified health claim is not FDA approval. It is a regulatory category that acknowledges some credible scientific evidence exists without reaching the threshold of significant scientific agreement — the standard required for full health claims. The European Food Safety Authority reviewed the same evidence and declined to approve any health claim at all, citing that bovine-cortex and soy-derived PS are different substances with potentially different biological activities and that results from studies of one cannot be generalized to the other.
The full picture: PS has a real and meaningful research base for specific populations, but the regulatory distinction is weaker than marketing implies. Presenting it honestly — as it is presented here — is more useful than either dismissing it or overclaiming it. A compound does not need FDA endorsement to be worth using. It needs accurate characterization of who it helps and how.
The Mechanisms: How PS Supports Cognitive Function
1. Membrane Integrity and Neuronal Signaling
PS is a required cofactor for protein kinase C (PKC) and Akt activation — two signaling pathways that directly govern neuronal survival, neurite growth, synaptic plasticity, and the formation of new synaptic connections. Without adequate PS in the inner membrane leaflet, these signaling pathways underperform. The practical effect of aging-related PS depletion is progressive degradation of the structural substrate for synaptic plasticity — the molecular foundation of memory formation and retention. Supplementation that maintains membrane PS levels preserves the functional capacity of these pathways in ways that slower-onset improvements in memory consolidation directly reflect.
2. Cholinergic Support
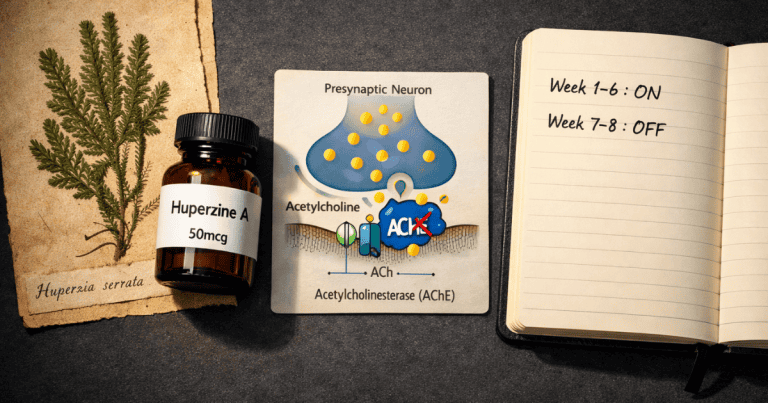
PS has demonstrated consistent effects on acetylcholine release in preclinical and human studies. It reverses age-dependent decreases in cortical acetylcholine release — documented directly in microdialysis studies — and supports the cholinergic system that governs the attentional and memory circuits most affected by aging. This cholinergic mechanism complements rather than duplicates Alpha-GPC’s direct choline substrate delivery: Alpha-GPC provides the raw material for acetylcholine synthesis; PS supports the membrane environment in which cholinergic neurons operate most effectively. Both increase cholinergic output, but through different and complementary mechanisms.
3. HPA Axis Modulation and Cortisol Blunting
PS has documented effects on the hypothalamic-pituitary-adrenal axis — specifically blunting both ACTH and cortisol responses to physical and psychological stress. Monteleone and colleagues (1992) demonstrated in a placebo-controlled trial that chronic PS administration significantly blunted the stress-induced activation of the HPA axis in healthy men. Multiple exercise studies confirmed this: BC-PS at 800mg/day moderated cortisol response to intense exercise-induced stress, and soy-PS at 600mg/day produced significant cortisol attenuation during moderate-intensity cycling. This HPA modulation overlaps mechanistically with Ashwagandha’s primary mechanism — but operates through a different pathway (membrane-level regulation of the HPA stress cascade rather than glucocorticoid receptor modulation), making the two genuinely complementary for individuals under chronic stress.
4. Dopamine and Noradrenaline Regulation
PS regulates release of dopamine and noradrenaline — neurotransmitters governing motivation, executive function, and the prefrontal cortex’s working memory and planning capacity. The dopaminergic regulation is particularly relevant for the attention and processing speed improvements observed in clinical trials, and may partially explain why PS research in ADHD populations (both children and adults) has produced positive results. This monoaminergic effect is a secondary mechanism compared to the membrane integrity and cholinergic pathways described above, but it contributes to the broader cognitive performance profile that PS’s clinical evidence demonstrates.
The Research: What the Clinical Trials Actually Show
The Crook 1991 Trial — The Benchmark Study
Crook and colleagues (1991) conducted the most influential PS trial in the literature — a randomized, double-blind, placebo-controlled study in 149 patients meeting criteria for age-associated memory impairment (AAMI). Participants received 100mg bovine cortex PS three times daily (300mg total) or placebo for 12 weeks. PS-treated patients improved significantly on computerized memory and learning tests, standard neuropsychological assessments, and clinical global ratings compared to placebo. Crucially, the greatest improvements occurred in the subgroup who performed at the lowest levels at baseline — suggesting PS has the most pronounced effects in those with the most room for improvement, consistent with a mechanism of restoring depleted membrane PS levels. This study formed the primary evidence base for the subsequent FDA qualified health claim.
The Cenacchi 1993 Multicenter Trial
Cenacchi and colleagues (1993) conducted a large-scale double-blind placebo-controlled multicenter trial in 494 elderly patients with cognitive decline — the largest PS trial in the literature. At 300mg/day BC-PS for 6 months, treated patients showed significant improvements in memory functions and behavioral parameters compared to placebo, with the improvements well-maintained through the assessment period. The scale of this trial — nearly 500 participants across multiple centers — gives it substantial statistical weight and reduces the confounding that affects smaller single-center studies.
Soy-Derived PS: The Sourcing Transition and Its Research Implications
The majority of the foundational PS clinical evidence — including the Crook and Cenacchi trials — used bovine cortex-derived PS (BC-PS). In the late 1990s, the supplement industry transitioned away from BC-PS due to concerns about prion transmission (BSE/mad cow disease risk from bovine brain material). All commercially available PS supplements today use plant-derived PS — primarily soy-derived (Soy-PS) or, more recently, sunflower-derived PS. This sourcing shift is the most clinically significant nuance in the PS literature and is frequently glossed over.
Soy-PS has a different fatty acid composition than BC-PS — it is predominantly paired with linoleic acid rather than the DHA-rich fatty acid chains of bovine brain-derived PS. The EFSA’s refusal to approve a health claim was based precisely on this: the two substances are not identical and results from BC-PS studies cannot be directly extrapolated. Soy-PS evidence exists and is generally positive, but the effect sizes appear smaller and the results more variable than the original BC-PS literature. The most rigorous Soy-PS study by Kato-Kataoka and colleagues (2010) in 78 elderly Japanese adults found significant memory improvements in the low-baseline subgroup — mirroring the Crook 1991 pattern — but not in the overall sample. The consistent pattern: PS effects are most detectable in those with the most baseline impairment.
Cortisol Blunting and Stress — The Monteleone Studies
Monteleone and colleagues (1992) demonstrated that chronic BC-PS administration significantly blunted the stress-induced HPA axis activation in healthy men — reducing both ACTH and cortisol responses to physical stress. This finding was extended by Starks and colleagues (2008), who found that soy-PS at 600mg/day for 10 days in a double-blind crossover trial produced significant cortisol attenuation during exercise stress, alongside improved performance on the Serial Subtraction Test. The EEG study by Baumeister and colleagues (2008) extended this finding to cognitive context: 42 days of PS supplementation produced significant reductions in Beta-1 cortical power in right frontal brain regions under induced stress — a neurophysiological signature of reduced stress-driven cognitive interference. For individuals whose primary cognitive performance limitation is stress-driven, this is a meaningful effect on a meaningful measurement.
ADHD and Attention: A Specific Application
Hirayama and colleagues (2013) conducted a randomized double-blind placebo-controlled trial of 200mg/day Soy-PS in 36 children with ADHD aged 4–14 who had not previously received pharmacological treatment. PS supplementation produced significant improvements in ADHD symptoms, short-term auditory memory, and inattention measures compared to placebo. This is one of the most cleanly designed PS studies in the modern literature and notable for demonstrating that PS effects on the dopaminergic and cholinergic systems translate into measurable behavioral improvements in a population defined by deficits in exactly those systems. For adults with attention difficulties who prefer non-pharmacological approaches, this evidence is worth noting — though extrapolation from the pediatric ADHD population to healthy adults requires appropriate caution.
The Honest Summary of the Evidence
PS has consistent evidence for memory improvement in older adults with age-related decline, a well-replicated cortisol blunting mechanism, and a meaningful cholinergic support effect. Effect sizes in healthy young adults without cognitive impairment are smaller and less consistent — the honest characterization is that PS does more for people who have more to recover than for people operating at their genetic ceiling. The sourcing shift from BC-PS to Soy-PS introduces genuine uncertainty about whether modern commercially available products replicate the effect sizes of the foundational trials. PS is most defensible as a long-term structural brain support compound — not as an acute cognitive enhancer, and not as a primary stack driver. It is the foundation beneath the foundation.
⬇ Free Download
Get the 7-Day Brain Optimization Protocol
The evidence-based behavioral and supplement framework for your first week of cognitive enhancement — covering sleep optimization, L-theanine + caffeine, creatine, Lion’s Mane, and the daily protocols that make them work. Completely free.
Join 2,000+ readers optimizing their cognitive performance. No spam, ever. Unsubscribe anytime.
Dosing Protocol: What the Evidence Supports
The clinical trial literature converges on 300mg/day as the standard dose for cognitive effects — administered as 100mg three times daily with meals in the majority of studies. This divided-dose protocol reflects PS’s status as a membrane nutrient that is absorbed and incorporated gradually rather than producing peak plasma concentrations that correlate with acute effects.
Unlike most compounds in this series where cycling is either required or recommended, cycling is not indicated for PS. It is a structural membrane nutrient, not a compound that acts on receptor systems that undergo downregulation. Consistent daily use indefinitely is the appropriate protocol — the same relationship as DHA supplementation, which PS pairs best with.
The PS + DHA Synergy — Why the Combination Matters
The most important sourcing consideration for PS — beyond the bovine vs. soy question — is the fatty acid composition. Brain-derived PS is naturally rich in DHA (docosahexaenoic acid), the omega-3 fatty acid most concentrated in neuronal membranes. The original BC-PS preparations were DHA-rich; commercial Soy-PS is predominantly linoleic acid. Some researchers argue that the reduced efficacy of Soy-PS versus BC-PS is at least partially attributable to the absence of DHA rather than the PS molecule itself. Several clinical trials have specifically tested PS combined with DHA (as PS-DHA or “PS omega-3”) and found superior effects to Soy-PS alone — particularly for memory in older adults with subjective memory complaints. The practical protocol implication: take soy-PS with DHA supplementation (1,000–2,000mg EPA+DHA daily from fish oil). The combination approximates the fatty acid composition of the original BC-PS preparations that produced the strongest clinical evidence.
What to Expect — Onset Timeline
Onset Timeline
Weeks 1–3: No noticeable cognitive effect expected. PS is being incorporated into neuronal membranes — a gradual structural process with no acute subjective signature.
Weeks 3–6: For those under significant stress, cortisol blunting effects may become apparent — reduced stress reactivity, easier recovery from demanding periods. For cognitive effects specifically, this timeline is variable.
Weeks 6–12: Cognitive improvements — primarily memory consolidation and recall — become detectable in clinical assessment. Most trials ran 12 weeks for this reason. Subjective experience of improvement at this stage is meaningful.
Beyond 12 weeks: Continued use maintains the membrane PS levels that underlie the cognitive benefit. This is not a compound where discontinuing after 12 weeks preserves the gains — stopping means membrane PS levels begin declining again toward baseline.
Safety Profile and Contraindications
Soy-derived PS has one of the strongest safety records of any nootropic compound in commercial use. The large-scale Cenacchi multicenter trial (494 participants, 6 months) reported no serious adverse events. Decades of widespread commercial use have not generated toxicity signals comparable to compounds with more aggressive pharmacological mechanisms. The primary safety considerations are drug interaction risks, not direct toxicity.
Anticholinergic medications: PS enhances cholinergic activity. This creates a pharmacodynamic interaction with medications that block acetylcholine — including antihistamines, bladder medications, and some antidepressants with anticholinergic properties. PS may reduce the effectiveness of these medications, and the interaction should be discussed with a prescriber.
Anticoagulants: Limited case evidence suggests PS may have mild blood-thinning effects. Individuals taking warfarin, heparin, or high-dose aspirin should monitor INR and consult their physician.
Soy allergy: Commercial Soy-PS is highly purified and contains negligible soy protein. Most individuals with soy protein allergies tolerate soy lecithin and soy-derived PS without reaction. However, those with severe soy anaphylaxis should use sunflower-derived PS as an alternative and confirm with their allergist.
GI effects at high doses: Doses above 300mg/day occasionally produce mild gastrointestinal discomfort — nausea or loose stools — particularly when taken on an empty stomach. The three-times-daily with-meals dosing protocol used in the clinical literature effectively mitigates this. Starting at 100mg/day and increasing over 2–3 weeks allows tolerance assessment.
Sourcing: What to Look For
Soy-derived PS is the standard and appropriate choice for the vast majority of users. Sunflower-derived PS is an emerging alternative for those avoiding soy — it has a similar phospholipid profile and preliminary evidence suggests comparable effects, though the research base is smaller. Bovine cortex PS is no longer commercially available for human consumption and should not be sought out.
What to verify on a label: PS content listed as elemental phosphatidylserine (not soy lecithin — lecithin contains only a fraction of PS), minimum 20% PS concentration for soy-based products, third-party purity testing and COA documentation. Products listing only “soy lecithin” or “phospholipid complex” without specifying PS percentage are not equivalent to the 100–300mg PS doses used in clinical trials.
The strongest commercial PS option for the cognitive performance + cortisol support application is a product that combines PS with DHA — either as a PS-DHA complex from marine sources (herring roe) or as separate soy-PS and fish oil taken together. If using separate products, take them simultaneously with a meal containing dietary fat for optimal absorption of both.
Stack Integration: Where PS Fits in the Full Protocol
PS belongs in the foundational layer of a nootropic protocol alongside DHA and creatine — compounds that work at the structural and metabolic substrate level rather than at the neurotransmitter modulation level. In the context of the full cognitive performance framework:
The structural layer — PS + DHA — maintains the membrane integrity and fatty acid composition that all other cognitive function depends on. The adaptogenic layer — Ashwagandha + Panax ginseng — normalizes the stress and vascular conditions under which cognition operates. The acute performance layer — L-theanine + caffeine and Alpha-GPC — delivers immediate session-level cognitive performance. PS and DHA make the substrate on which everything else operates.
Integrated Morning Stack Protocol
On waking
Panax ginseng 200–400mg
60 min after waking
Caffeine 100mg + L-Theanine 200mg
With breakfast
PS 100mg + DHA 1000–2000mg + Creatine 5g + Lion’s Mane 1000mg
With lunch
PS 100mg
Evening
Ashwagandha 300–600mg + Magnesium L-Threonate 1500mg + PS 100mg with dinner
Frequently Asked Questions About Phosphatidylserine
What does phosphatidylserine do for the brain?
PS is a structural component of neuronal membranes that supports multiple cognitive functions simultaneously. It maintains membrane integrity for the signaling pathways that govern neuronal survival and synaptic plasticity (PKC, Akt), supports acetylcholine release in the cholinergic circuits governing memory and attention, and blunts ACTH and cortisol responses to stress through HPA axis modulation. The practical effects these mechanisms produce — better memory consolidation and recall, reduced stress-driven cognitive impairment, and preserved attention — build over 6–12 weeks of consistent supplementation. PS does not produce acute cognitive effects. It is structural brain maintenance, not an acute enhancer.
What is the difference between bovine and soy phosphatidylserine?
The foundational PS research used bovine cortex-derived PS (BC-PS), which is DHA-rich in its fatty acid composition — closely matching the phospholipid profile of human neuronal membranes. The supplement industry transitioned to soy-derived PS (Soy-PS) in the late 1990s due to BSE/prion concerns with bovine brain material. Soy-PS has a different fatty acid composition (predominantly linoleic acid rather than DHA). The European Food Safety Authority declined to approve health claims for PS partly on the basis that BC-PS and Soy-PS are different substances. Soy-PS evidence is positive but shows smaller effect sizes than the original BC-PS literature. The practical solution: take soy-PS alongside DHA supplementation to approximate the fatty acid environment of BC-PS. Bovine cortex PS is not commercially available and should not be sought out.
How long does phosphatidylserine take to work?
PS produces no acute cognitive effects — it is incorporated into neuronal membranes gradually over weeks, not absorbed and acting within hours like caffeine or ginseng. Clinical trials consistently used 6–12 week treatment periods to detect cognitive improvements. The realistic timeline: weeks 3–6 for cortisol blunting and stress resilience effects to become apparent; weeks 6–12 for memory consolidation and recall improvements to become detectable. The 12-week mark is the appropriate first assessment point for cognitive effects. PS is a compound where the decision to continue should be made at 12 weeks based on subjective cognitive and stress assessment — not abandoned at 3 weeks because nothing acute has occurred.
Can I take phosphatidylserine with Ashwagandha and Panax ginseng?
Yes — the three compounds occupy different mechanistic layers and are genuinely complementary. Ashwagandha addresses HPA axis cortisol architecture through glucocorticoid receptor modulation. Panax ginseng addresses vascular delivery, cholinergic substrate, and working memory through NO-mediated and cholinergic mechanisms. PS addresses the structural membrane integrity and cortisol blunting that underlies everything else. No clinically significant adverse interactions exist between these three compounds at standard doses. Taking all three simultaneously is appropriate once each has been individually established — the recommended sequencing is Ashwagandha first (weeks 1–8), ginseng second (weeks 6–14), PS ongoing from the start given its benign safety profile and long onset timeline.
Does phosphatidylserine need to be cycled?
No. PS is a structural membrane nutrient, not a compound that modulates receptor systems subject to downregulation or tolerance. It does not require cycling. Consistent daily use is both safe and appropriate — stopping supplementation means brain PS levels gradually decline back toward baseline, removing the structural benefits that accumulated over the dosing period. This is qualitatively similar to DHA: consistent supplementation maintains the membrane composition that supports cognitive function; discontinuation allows depletion to resume. For this reason, PS is best treated as a permanent addition to a cognitive health protocol rather than a cycling compound.
Scientific References
- Crook, T.H., et al. (1991). Effects of phosphatidylserine in age-associated memory impairment. Neurology, 41(5), 644–649. PubMed
- Cenacchi, T., et al. (1993). Cognitive decline in the elderly: a double-blind, placebo-controlled multicenter study on efficacy of phosphatidylserine administration. Aging (Milano), 5(2), 123–133. PubMed
- Monteleone, P., et al. (1992). Blunting by chronic phosphatidylserine administration of the stress-induced activation of the hypothalamo-pituitary-adrenal axis in healthy men. European Journal of Clinical Pharmacology, 42(4), 385–388. PubMed
- Kato-Kataoka, A., et al. (2010). Soybean-derived phosphatidylserine improves memory function of the elderly Japanese subjects with memory complaints. Journal of Clinical Biochemistry and Nutrition, 47(3), 246–255. PMC
- Starks, M.A., et al. (2008). The effects of phosphatidylserine on endocrine response to moderate intensity exercise. Journal of the International Society of Sports Nutrition, 5, 11. PMC
- Baumeister, J., et al. (2008). Influence of phosphatidylserine on cognitive performance and cortical activity after induced stress. Nutritional Neuroscience, 11(3), 103–110. PubMed
- Hirayama, S., et al. (2013). The effect of phosphatidylserine administration on memory and symptoms of attention-deficit hyperactivity disorder: a randomised, double-blind, placebo-controlled clinical trial. Journal of Human Nutrition and Dietetics, 27(Suppl 2), 284–291. PubMed
- Kingsley, M. (2006). Effects of phosphatidylserine supplementation on exercising humans. Sports Medicine, 36(8), 657–669. PubMed
- Kim, H.Y., Huang, B.X., Spector, A.A. (2014). Phosphatidylserine in the brain: metabolism and function. Progress in Lipid Research, 56, 1–18. PubMed
- FDA (2003). Qualified Health Claim: Phosphatidylserine and Cognitive Dysfunction and Dementia. FDA.gov