The Best Supplements for Sleep: What the Evidence Actually Shows
Medical Disclaimer: The information in this article is for educational purposes only and does not constitute medical advice. Sleep disorders including insomnia disorder, sleep apnea, and circadian rhythm disorders require professional evaluation. Supplements interact with medications — consult a qualified healthcare provider before beginning any regimen, especially if you take prescription medications or have pre-existing conditions. Individual responses vary significantly.
The sleep supplement market is one of the most aggressively marketed segments of the entire supplement industry — and one of the most reliably misleading. Walk through any pharmacy or supplement retailer and you will find dozens of products confidently promising deep, restorative sleep. Most of them are either pharmacologically ineffective for the claimed purpose, genuinely sedating in ways that impair sleep quality while inducing unconsciousness, or addressing a timing problem when the actual issue is depth or stress. The difference matters significantly — a sedative that puts you to sleep faster while suppressing REM produces worse cognitive outcomes than not taking anything at all.
After 18+ years personally testing sleep compounds and researching the literature, I have found a small number of supplements with genuinely compelling evidence for improving specific, meaningful aspects of sleep quality — SWS depth, sleep spindle density, cortisol management, or sleep onset neurochemistry — through mechanisms that align with the biology of what sleep is actually trying to accomplish. Those compounds are what this guide covers. Everything else — the proprietary blends with underdosed ingredients, the GABA supplements that cannot cross the blood-brain barrier at oral doses, the 10mg melatonin gummies, the “sleep support” formulas with 40 ingredients — is filtered out by the same evidence standard applied throughout NeuroEdge Formula.
This is the final guide in the Sleep hub, synthesizing the supplementation layer that works on top of the behavioral protocols in the complete sleep guide, the sleep architecture science in the architecture guide, and the sleep-cognition connection in the cognitive performance guide.
The Evidence Framework: What “Best” Actually Means for Sleep Supplements
Before reviewing individual compounds, the framework for evaluating sleep supplements is essential — because the category is uniquely prone to conflating sedation with sleep quality, and the two are not the same thing.
A sedative that produces unconsciousness faster is not a sleep quality enhancer. Alcohol, antihistamines (diphenhydramine — the active ingredient in most OTC sleep aids), and benzodiazepines all reduce sleep onset latency while simultaneously suppressing the SWS and REM stages that constitute restorative sleep. You fall asleep faster and wake up feeling worse — which is the exact pharmacological profile of the most widely used OTC sleep aids. The compounds in this guide are evaluated on a different standard: do they improve the depth, composition, or cognitive restoration of sleep, not merely the speed of unconsciousness onset?
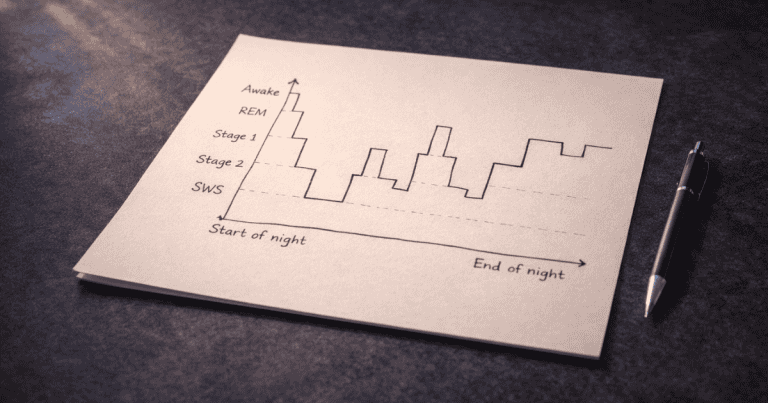
The four sleep quality dimensions this guide evaluates against: SWS depth and duration (the primary physical restoration and memory consolidation mechanism), sleep spindle density (the N2 mechanism for cognitive maintenance and sensory suppression), REM protection and duration (emotional processing, creativity, procedural memory), and sleep onset quality — specifically the alpha-wave parasympathetic transition rather than sedative unconsciousness. Compounds are rated by their evidence for improving one or more of these dimensions without impairing the others.
Tier 1 — The Core Sleep Stack: Strongest Evidence, Direct Mechanisms
Magnesium L-Threonate — The Highest-Priority Sleep Supplement
Magnesium L-Threonate occupies a unique position in the sleep supplement landscape: it is the only magnesium form demonstrated to meaningfully cross the blood-brain barrier and elevate brain magnesium levels — and brain magnesium is a direct regulator of the NMDA receptors and GABAergic circuits that govern SWS induction, sleep spindle generation, and sleep maintenance. Most magnesium supplements — oxide, citrate, glycinate — support body magnesium status without specifically elevating brain magnesium, which is why MgT produces effects on sleep architecture that other magnesium forms do not replicate.
Research by Slutsky and colleagues found that MgT supplementation elevated brain magnesium levels by 15% above the ceiling achievable with conventional magnesium supplementation — producing significant improvements in synaptic density, sleep spindle activity, and memory performance. The sleep spindle enhancement is a direct, mechanistically specific benefit: sleep spindles are the thalamo-cortical oscillations that coordinate hippocampal memory replay with neocortical storage during N2 and SWS — meaning MgT improves sleep quality in a way that directly amplifies the cognitive dividend of the sleep it enhances.
In my 18+ years of testing sleep compounds, MgT produces the most consistently noticeable subjective sleep quality improvement of any supplement I have assessed — particularly in the dimension of feeling genuinely cognitively restored rather than merely rested. The difference between adequate sleep with and without MgT is subtle but cumulative; over weeks, the compounding of improved sleep spindle consolidation becomes measurable in actual learning retention and cognitive performance.
Evidence level: Strong animal and human mechanistic studies — Level 2/3
Sleep dimensions improved: SWS induction, sleep spindle density, sleep maintenance, sleep quality subjective scores
Dose: 1,500–2,000mg daily in divided doses — 1,000mg morning, 500–1,000mg 1–2 hours before bed
Timeline: Sleep quality improvements within 1–2 weeks; full synaptic effects at 8–12 weeks
Full protocol: Magnesium L-Threonate guide
Ashwagandha KSM-66 — Cortisol-Driven Sleep Disruption, Solved
Ashwagandha KSM-66 is the most evidence-supported botanical for addressing the most common cause of poor sleep quality in cognitively active adults: elevated evening cortisol from chronic stress. Cortisol activates the HPA axis arousal systems that directly oppose the VLPO suppression required for sleep onset and SWS maintenance — producing the pattern of lying awake with a racing mind, waking at 3–4am, and obtaining light, fragmented sleep even when total duration appears adequate.
Research by Langade and colleagues conducted a randomized, double-blind, placebo-controlled trial finding that Ashwagandha KSM-66 at 300mg twice daily for 10 weeks produced significant improvements in sleep onset latency (time to fall asleep), total sleep time, sleep efficiency, and morning alertness — with the improvements correlated with reductions in cortisol and serum anxiety measures, confirming the HPA axis mechanism. This is not a sedative effect — Ashwagandha does not cause drowsiness or impair next-day alertness. It normalizes the stress-driven neurochemical dysregulation that prevents normal sleep from occurring.
Evidence level: Multiple RCTs — Level 1/2
Sleep dimensions improved: Sleep onset latency, SWS depth (through cortisol reduction), total sleep time, sleep efficiency, morning alertness
Dose: 300–600mg KSM-66 extract in the evening, 1–2 hours before bed
Timeline: Initial improvements within 2–4 weeks; full HPA axis normalization at 8–10 weeks
Full protocol: Ashwagandha guide
L-Theanine — Sleep Onset Without Sedation
L-theanine at 200–400mg is the most evidence-supported non-sedating sleep onset supplement available — and the distinction between non-sedating and sedating is critical for understanding why it is the preferred first-line supplement for sleep onset difficulty over antihistamines, high-dose melatonin, and most proprietary “sleep blend” formulas.
L-theanine promotes alpha-wave brain activity — the same relaxed, alert mental state that characterizes mindfulness practice — through enhancement of GABAergic inhibitory tone and inhibition of excitatory glutamate activity. It does not cause drowsiness, does not impair next-day alertness, does not suppress SWS or REM, and does not produce tolerance or dependency with nightly use. Research on L-theanine and sleep quality found improvements in sleep efficiency and reduced sleep fragmentation — consistent with the alpha-wave mechanism reducing the cognitive hyperarousal that both delays sleep onset and fragments sleep architecture.
L-theanine pairs synergistically with both MgT and Ashwagandha — addressing sleep onset neurochemistry (L-theanine), sleep depth and spindle quality (MgT), and the cortisol substrate driving hyperarousal (Ashwagandha) through three non-overlapping mechanisms. The three compounds together produce more comprehensive sleep quality improvement than any single compound achieves alone.
Evidence level: Multiple clinical studies — Level 2
Sleep dimensions improved: Sleep onset quality, sleep efficiency, sleep fragmentation reduction
Dose: 200–400mg, 45–60 minutes before bed
Timeline: Acute effects from the first dose
Notes: Non-sedating, non-habit-forming, compatible with nightly use. Does not cause next-day grogginess.
Free Download
Get the 7-Day Brain Optimization Protocol
The evidence-based diet, sleep, and supplement framework for your first week of cognitive enhancement — completely free.
Join 2,000+ readers optimizing their cognitive performance. Unsubscribe anytime.
Tier 2 — Supporting Sleep Stack: Targeted Applications
Melatonin — For Circadian Timing, Not Sleep Depth
Melatonin is the most widely used sleep supplement globally — and the most consistently misunderstood. It is a circadian timing signal produced by the pineal gland in response to darkness, signaling the brain that it is biologically nighttime. It is not a sedative. It does not directly improve SWS depth, REM duration, or sleep architecture quality beyond their circadian-appropriate levels. Understanding this distinction is what determines whether melatonin is an appropriate supplement for a specific sleep problem.
Appropriate applications: Jet lag — low-dose melatonin (0.5–1mg) taken at the target destination bedtime shifts the circadian clock toward the new time zone, reducing adjustment time by 1–2 days. Delayed sleep phase syndrome — the night owl pattern of naturally feeling sleepy very late and waking very late — can be gradually advanced by taking 0.5mg 5–6 hours before the target bedtime, progressively shifting the phase earlier over weeks. Shift work — melatonin taken before daytime sleep helps shift workers initiate sleep during the biologically inappropriate daytime circadian phase.
Inappropriate applications: General sleep quality improvement in normally-timed individuals. For most adults who simply want deeper, more restorative sleep — and whose sleep timing is reasonably aligned with their circadian phase — melatonin adds little beyond placebo effect. The compounds that actually improve sleep depth and quality (MgT, Ashwagandha, L-theanine) are the appropriate tools for this goal.
Dose note: The 5–10mg doses commonly marketed in OTC products are supraphysiological — the brain naturally produces 0.1–0.3mg. Research consistently shows that 0.5mg is as effective as higher doses for circadian phase-shifting applications and produces fewer next-day side effects. Higher doses may desensitize melatonin receptors with regular use and shift circadian timing in ways that worsen sleep problems.
Evidence level: Multiple RCTs for circadian applications — Level 1 for jet lag/phase shift; weak evidence for general sleep quality
Dose: 0.5–1mg for circadian applications; taken 5–6 hours before target bedtime for phase advancement
Avoid: 5–10mg doses, nightly use without circadian indication
DHA (Omega-3) — The Structural Foundation
DHA at 1,000–2,000mg daily is less a direct sleep supplement than a foundational nutritional requirement for brain cell membrane health — but its impact on sleep quality is meaningful enough to warrant inclusion in any comprehensive sleep optimization stack. DHA deficiency is associated with reduced melatonin production, increased neuroinflammation that disrupts sleep architecture, and reduced hippocampal neurogenesis that sleep is partly responsible for supporting.
Research on omega-3 supplementation and sleep quality in children found that DHA supplementation significantly improved sleep duration and reduced waking episodes — with the mechanism involving both melatonin synthesis pathway support and reduction of neuroinflammatory signaling that disrupts sleep maintenance. For adults whose omega-3 intake from dietary fatty fish is insufficient, DHA supplementation addresses a nutritional substrate of sleep quality that more targeted sleep supplements cannot compensate for.
Evidence level: Multiple studies — Level 2
Sleep dimensions improved: Sleep continuity, sleep duration, melatonin synthesis support
Dose: 1,000–2,000mg DHA daily with largest meal
Timeline: 4–8 weeks for membrane incorporation effects
What to Avoid: The Popular Sleep Supplements That Don’t Work (Or Actively Harm Sleep)
As important as knowing what to take is knowing what to avoid — particularly the compounds that are widely marketed with confident sleep claims but produce either no benefit or genuine harm to sleep quality.
Diphenhydramine (Benadryl, ZzzQuil, Unisom): The active ingredient in most OTC sleep aids. A first-generation antihistamine that produces sedation through H1 receptor blockade — not through any mechanism that improves sleep architecture. Develops tolerance within 3–4 nights, suppresses REM sleep, and produces next-day cognitive impairment (“antihistamine hangover”) through residual H1 blockade of the histaminergic arousal system. Regular use is associated with accelerated cognitive aging — a finding that should give anyone using it regularly serious pause.
High-dose melatonin (5–10mg): As described above — supraphysiological doses that may desensitize receptors and produce circadian timing disruption without improving sleep depth or quality. The 10mg gummy market is a triumph of marketing over pharmacology.
Oral GABA supplements: GABA is the primary inhibitory neurotransmitter and the obvious theoretical candidate for a sleep supplement — which is why dozens of sleep products contain it. The problem is that GABA has very poor blood-brain barrier penetration at oral doses, meaning supplemental GABA does not meaningfully raise brain GABA levels. The compounds that effectively enhance GABAergic tone in the brain — MgT, L-theanine, Ashwagandha — do so through mechanisms that cross the blood-brain barrier (NMDA modulation, direct GABA receptor enhancement, and HPA axis regulation respectively), not through oral GABA delivery.
Valerian root: One of the most historically used botanical sleep aids with one of the most disappointingly weak evidence profiles. Multiple meta-analyses of valerian clinical trials have found inconsistent results that do not support reliable efficacy for sleep quality or onset. Some individuals report subjective benefit, but the controlled trial evidence does not support recommending it over the compounds in Tier 1 with significantly stronger mechanistic and clinical evidence.
The Complete Sleep Supplement Stack: Integration and Timing
The complete evidence-based sleep supplement stack integrates Tier 1 and Tier 2 compounds into a coherent daily protocol aligned with the sleep quality dimensions each compound addresses.
📋 Complete Sleep Supplement Protocol
MORNING — with breakfast
Magnesium L-Threonate 1,000mg + DHA 1,000–2,000mg
EVENING — 60–90 minutes before bed
Magnesium L-Threonate 500–1,000mg + Ashwagandha KSM-66 300–600mg + L-theanine 200–400mg
SITUATIONAL — jet lag or delayed sleep phase only
Melatonin 0.5mg taken 5–6 hours before target bedtime for phase advancement, or at target destination bedtime for jet lag
Beginner Introduction Sequence
For individuals new to sleep supplementation, introducing all compounds simultaneously is not necessary. The sequenced approach produces the clearest feedback on what is working.
Week 1–2: L-theanine 200mg before bed. Produces immediate, perceptible effects on sleep onset quality — the most useful first signal that supplementation is affecting sleep neurochemistry. Most people notice the difference within the first 3–5 nights.
Week 3–4: Add Magnesium L-Threonate at the full daily dose (morning and evening split). Sleep depth and morning cognitive restoration improvements begin within the first 1–2 weeks. If magnesium intake from diet is significantly deficient, this can be a noticeably impactful addition.
Week 5+: Add Ashwagandha KSM-66 if stress, anxiety, or the 3am waking pattern are present. Its cortisol-normalizing effects develop over 4–6 weeks — the impact on sleep quality compounds with the MgT foundation already established. Add DHA if dietary fatty fish consumption is consistently below 2 servings per week.
At week 12, with the complete stack in place and the behavioral protocols from the complete sleep guide applied consistently, the full integrated sleep optimization protocol is operating — and the cognitive performance benefits described in the cognitive performance guide are fully accessible.
Frequently Asked Questions About Sleep Supplements
What is the best supplement for deep sleep?
Magnesium L-Threonate is the best-evidenced supplement for improving slow wave (deep) sleep quality through a direct neurobiological mechanism. Unlike other magnesium forms, MgT crosses the blood-brain barrier to elevate brain magnesium levels, which directly supports the GABAergic SWS induction circuits and thalamo-cortical sleep spindle generation that constitute deep sleep’s restorative function. The sleep spindle enhancement is particularly meaningful — spindles are the mechanism through which hippocampal memory replay is coordinated with neocortical storage during deep sleep, making MgT’s spindle support a direct memory consolidation benefit alongside the sleep depth improvement. Ashwagandha KSM-66 is the best-evidenced supplement for restoring deep sleep that is being disrupted by elevated cortisol from chronic stress — its HPA axis normalization removes the primary biological obstacle to SWS depth in stressed individuals. For most cognitively active adults, combining both compounds addresses the two most common modifiable causes of insufficient deep sleep: suboptimal brain magnesium and cortisol-driven sleep fragmentation.
Is melatonin safe to take every night?
Melatonin is generally considered safe for short-term use, but nightly long-term use raises concerns that are underappreciated given how routinely it is recommended. Melatonin supplementation suppresses the brain’s endogenous melatonin production through feedback regulation — with evidence that chronic supplementation at common commercial doses (3–10mg) can reduce natural melatonin secretion over time. More significantly, nightly use at doses that alter circadian timing (which includes most commercial doses) can progressively shift sleep-wake timing in ways that require continued supplementation to maintain — a functional dependency mechanism distinct from sedative tolerance but similarly problematic. The most evidence-supported approach to melatonin is use for specific, time-limited circadian applications (jet lag, shift work adaptation, phase correction) at the lowest effective dose (0.5–1mg) rather than as a nightly sleep supplement. For nightly sleep quality support, the compounds that improve sleep architecture rather than timing — MgT, Ashwagandha, L-theanine — are more appropriate and have better long-term safety profiles for regular use.
What is the difference between Magnesium L-Threonate and Magnesium Glycinate for sleep?
Magnesium glycinate and Magnesium L-Threonate are both well-absorbed magnesium forms with good tolerability, but they serve different functions and should not be considered interchangeable for sleep optimization. Magnesium glycinate is an excellent form for correcting systemic magnesium deficiency — it is highly bioavailable, gentle on the digestive system, and effectively raises serum and tissue magnesium levels. It produces general relaxation and muscle tension reduction that many people find beneficial for sleep onset. However, magnesium glycinate does not meaningfully cross the blood-brain barrier at oral doses, so it does not significantly elevate brain magnesium levels or produce the specific thalamo-cortical sleep spindle and NMDA receptor optimization effects that brain magnesium provides. Magnesium L-Threonate was specifically designed to cross the blood-brain barrier — the threonate transport mechanism carries it into the brain in a way that other magnesium chelates do not achieve. For sleep quality effects that operate through brain magnesium mechanisms (sleep spindle density, NMDA receptor optimization, synaptic density), MgT is the appropriate choice. For correcting systemic magnesium deficiency and general relaxation effects, magnesium glycinate is effective and less expensive. Many individuals benefit from both — glycinate for systemic status and MgT for the specific cognitive and sleep architecture effects.
Can I take L-theanine and Ashwagandha together for sleep?
Yes — L-theanine and Ashwagandha are complementary rather than redundant for sleep quality, addressing different neurobiological mechanisms without overlap or interaction. L-theanine acts acutely on sleep onset by promoting alpha-wave brain activity through GABAergic enhancement and glutamate inhibition — reducing the cognitive hyperarousal of a busy mind without sedation. Its effects are present within the same dosing session. Ashwagandha acts on the HPA axis over weeks — normalizing cortisol production patterns to remove the chronic stress-driven neurochemical obstacle to sleep onset and SWS depth. The two compounds together address both the acute (cognitive hyperarousal at bedtime) and the chronic (elevated cortisol from sustained stress) contributions to poor sleep quality in a way that neither compound alone fully achieves. When adding Magnesium L-Threonate’s sleep spindle and SWS support, the three-compound combination — L-theanine for onset neurochemistry, Ashwagandha for cortisol management, MgT for sleep architecture depth — represents the most comprehensive evidence-based sleep supplement stack available without prescription intervention.
Do sleep supplements replace good sleep hygiene?
No — sleep supplements optimize the neurochemical conditions within which sleep hygiene behaviors produce their effects. They do not compensate for the circadian disruption of inconsistent sleep timing, the SWS suppression of a too-warm bedroom, the REM impairment of evening alcohol, or the adenosine dynamic disruption of late-afternoon caffeine. A person taking MgT, Ashwagandha, and L-theanine while sleeping on an inconsistent schedule in a warm, light-polluted room after two evening drinks will sleep worse than a person taking nothing while maintaining consistent timing, a cool dark bedroom, and alcohol-free evenings. The supplement stack amplifies what good sleep hygiene produces — it does not substitute for it. The most effective sleep optimization approach applies the behavioral foundation of the complete sleep guide first, then adds the supplement layer on top of a stable behavioral foundation. This sequencing produces the clearest signal about what each intervention is contributing and ensures the supplements are operating on a biological substrate that allows their effects to be fully expressed.
The Evidence-Based Sleep Stack: What It Actually Produces
The three-compound core stack — Magnesium L-Threonate, Ashwagandha KSM-66, and L-theanine — is not a collection of sleep pills. It is a targeted intervention on three distinct neurobiological mechanisms that most commonly stand between the sleep you are getting and the sleep your brain is capable of producing with optimal support: brain magnesium insufficiency limiting SWS depth and spindle quality, chronic cortisol elevation fragmenting sleep architecture and delaying onset, and cognitive hyperarousal blocking the smooth neurochemical transition into deep sleep that the biology is otherwise prepared to make.
Applied on top of the behavioral protocols across this hub — consistent timing, morning light, temperature optimization, caffeine discipline, alcohol avoidance — this stack produces a sleep quality that most cognitively active adults have not experienced since early adulthood. Not deeper unconsciousness — genuinely more restorative architecture: more SWS cycles completing their glymphatic clearance and memory consolidation function, more REM completing its emotional processing and creative integration, and a cognitive baseline the next morning that reflects what adequate, high-quality sleep is actually capable of providing.
For the complete behavioral protocol to pair with this supplement stack, see the complete sleep guide. For the sleep architecture science that explains why each stage matters, see the sleep architecture guide. For the cognitive performance reasons this all matters, see the sleep and cognitive performance guide.
References
- Slutsky, I., et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron, 65(2), 165–177. PubMed
- Langade, D., et al. (2019). Efficacy and safety of Ashwagandha root extract in insomnia and anxiety: A double-blind, randomized, placebo-controlled study. Cureus, 11(9), e5797. PubMed
- Rao, T.P., et al. (2015). In search of a safe natural sleep aid: L-theanine. Journal of the American College of Nutrition, 34(4), 436–447. PubMed
- Montgomery, P., et al. (2014). Fatty acids and sleep in UK children: Subjective and pilot objective sleep results from the DOLAB study. Journal of Sleep Research, 23(4), 364–388. PubMed
- Buscemi, N., et al. (2005). The efficacy and safety of exogenous melatonin for primary sleep disorders. Journal of General Internal Medicine, 20(12), 1151–1158. PubMed
- Ferracioli-Oda, E., et al. (2013). Meta-analysis: Melatonin for the treatment of primary sleep disorders. PLOS ONE, 8(5), e63773. PubMed
- Xie, L., et al. (2013). Sleep drives metabolite clearance from the adult brain. Science, 342(6156), 373–377. PubMed
- Ebrahim, I.O., et al. (2013). Alcohol and sleep I: Effects on normal sleep. Alcoholism: Clinical and Experimental Research, 37(4), 539–549. PubMed
- Gray, S.L., et al. (2015). Cumulative use of strong anticholinergics and incident dementia. JAMA Internal Medicine, 175(3), 401–407. PubMed
Tags: best supplements for sleep, sleep supplements, Magnesium L-Threonate sleep, Ashwagandha sleep supplement, L-theanine sleep, melatonin for sleep, deep sleep supplements, sleep quality supplements, natural sleep aids, sleep supplement stack, DHA sleep, sleep spindle supplements, cortisol sleep supplement, non-sedating sleep supplement, evidence-based sleep supplements
About Peter Benson
Peter Benson is a cognitive enhancement researcher and mindfulness coach with 18+ years of personal and professional experience in nootropics, neuroplasticity, and sleep optimization protocols. He has personally coached hundreds of individuals through integrated cognitive performance programs combining evidence-based sleep strategies with targeted supplementation. NeuroEdge Formula is his platform for sharing rigorous, safety-first cognitive enhancement guidance.