Magnesium L-Threonate: Benefits, Dosage, and What the Research Actually Shows
Affiliate Disclosure: Some links on this page are affiliate links. If you purchase through them, NeuroEdge Formula earns a small commission at no extra cost to you. Peter only recommends products he has personally tested and that meet the evidence standards of this site.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Magnesium L-Threonate may interact with antibiotics, bisphosphonates, and diuretics. The tolerable upper intake level for supplemental magnesium from the NIH is 350mg elemental magnesium daily — total supplemental magnesium across all forms should remain within this range. Consult a qualified healthcare provider before use if you take prescription medications or have kidney disease. Peter Benson is a cognitive enhancement researcher, not a medical doctor.
| What it is | A form of magnesium developed at MIT specifically to cross the blood-brain barrier — the only commercially available magnesium compound with documented ability to meaningfully raise brain magnesium concentrations via oral supplementation. Addresses both brain magnesium deficiency and the NMDA receptor gating mechanism underlying synaptic plasticity. |
| Why it’s unique | Standard magnesium supplements (glycinate, oxide, citrate) raise systemic magnesium but cross the blood-brain barrier poorly — even a 150–200% increase in plasma magnesium only raises CSF magnesium by 10–19%. Magnesium L-Threonate uniquely penetrates the CNS, reaching the neurons where magnesium’s cognitive effects occur. |
| Landmark finding | Liu et al. (2016): 2,000mg Magtein® daily for 12 weeks reversed approximately 9 years of age-related cognitive decline in adults aged 50–70. Published in the Journal of Alzheimer’s Disease — the most striking single cognitive finding in the MgT literature. |
| Standard dose | 2,000mg Magtein® daily (providing approximately 144mg elemental magnesium) — taken in the evening. Evening timing is important: MgT has documented sleep quality benefits that work synergistically with its cognitive mechanism via overnight memory consolidation. |
| Critical distinction | Magtein® (branded MgT, the form used in clinical trials) vs generic “magnesium L-threonate” powder. The clinical evidence was generated with Magtein® — the specific salt form, particle size, and purity matter. Unverified generic MgT has no confirmed clinical equivalence. |
| Deficiency prevalence | Approximately 48% of Americans fail to meet the estimated average requirement for magnesium from diet alone. This makes magnesium deficiency one of the most prevalent nutritional gaps in Western populations — and one of the most cognitively consequential. |
| Peter’s protocol | 2,000mg Magtein® with dinner — 30 minutes before the main sleep window. 3+ years continuous use. The compound Peter considers the most underappreciated in the intermediate cognitive protocol. |
Most people taking magnesium are taking the wrong form for cognitive purposes — and most people who should be taking it are not taking it at all. This is a compound with unusually strong mechanistic credentials, the most striking age-related cognitive reversal finding in the nootropic literature (approximately 9 years of cognitive decline reversed in 12 weeks in the Liu et al. trial), and a brain-penetration advantage so specific that it separates it entirely from the category of magnesium supplementation most people are familiar with. It also addresses a deficiency that affects approximately half the Western adult population and that impairs the effectiveness of every other neuroplasticity intervention in the stack.
The reason Magnesium L-Threonate remains underappreciated is partly because it operates slowly and structurally — its synaptic density mechanism is cumulative, not acute — and partly because the magnesium category is dominated by commodity thinking. People assume magnesium is magnesium, choose the cheapest option, and then never understand why brain-specific cognitive benefits don’t materialise from a compound that does not meaningfully reach the brain. The threonate carrier is not a marketing distinction — it is what makes the difference between a magnesium supplement and a brain magnesium supplement.
This guide covers the NMDA receptor gating mechanism, the MIT synaptic density research, the clinical evidence, the sleep–cognition dual benefit that makes evening timing optimal, and the Magtein® quality distinction that the evidence actually supports. For the broader neuroplasticity context, see the Brain Health & Longevity hub.
Mechanism: NMDA Receptors, Synaptic Plasticity, and Why Form Matters
The NMDA Receptor Gating Role of Magnesium
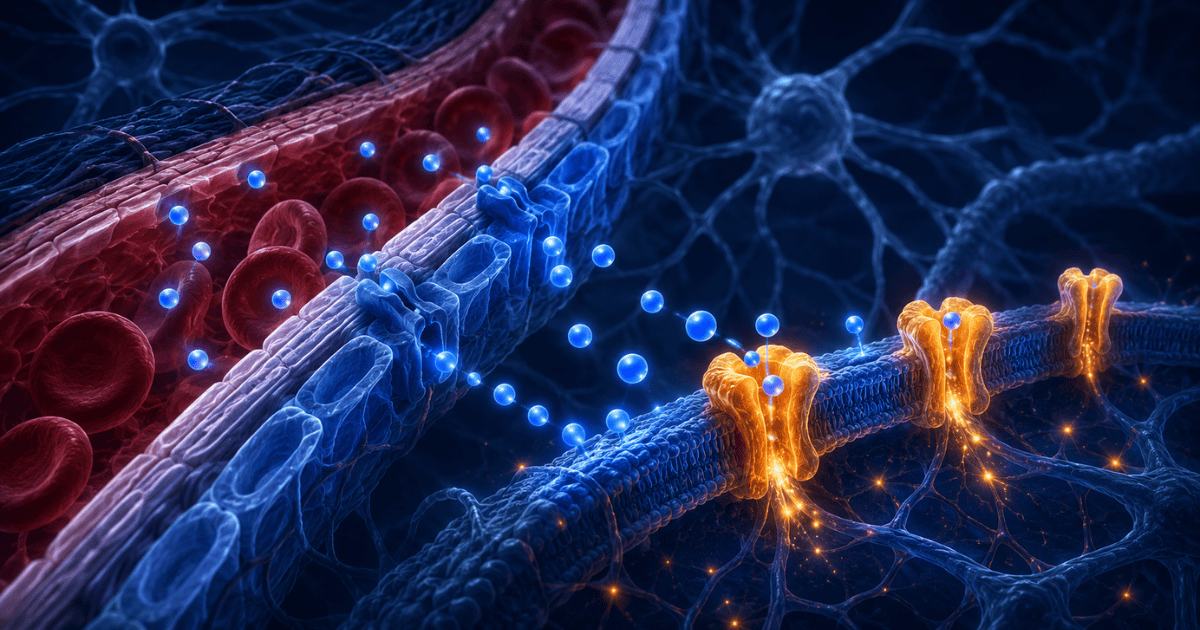
NMDA receptors are the molecular switches through which long-term potentiation (LTP) — the cellular mechanism of memory formation — occurs. At resting membrane potential, NMDA receptors are blocked by a magnesium ion in the channel pore. This blockade is voltage-dependent: when a neuron is sufficiently depolarised by incoming signals, the magnesium block is relieved, the NMDA receptor opens, calcium enters, and LTP is initiated. Brain magnesium concentration therefore functions as a gain control for synaptic plasticity — lower brain magnesium means the NMDA receptor threshold is harder to reach and LTP is less readily triggered. Higher brain magnesium means the gating mechanism is precisely tuned, enabling the discrimination between meaningful signals and noise that underlies efficient memory encoding.
Synaptic Density — The MIT Finding
Slutsky et al. (2010), published in Neuron, documented that elevating brain magnesium concentrations using MgT in animal models produced a significant increase in hippocampal synaptic density — the number of functional synaptic connections — alongside improvements in both short-term and long-term memory. This is the mechanistically important finding: MgT does not merely optimise existing synaptic function, it increases the structural density of the synaptic network itself. More synapses means more capacity for memory storage, more parallel processing, and greater cognitive resilience. This publication is why MgT attracted serious scientific attention and why the subsequent human trials were funded.
Why Standard Magnesium Cannot Replicate This
The blood-brain barrier actively regulates magnesium transport into the CNS — it cannot be bypassed by simply flooding the bloodstream with magnesium. Research on magnesium transport has confirmed that even a 150–200% increase in plasma magnesium concentration only produces a 10–19% increase in CSF magnesium. Standard magnesium forms (glycinate, oxide, citrate, malate) are effective at correcting systemic deficiency and have valuable peripheral nervous system and muscle function benefits — but they do not meaningfully raise brain magnesium concentrations. The threonate carrier in MgT appears to facilitate active transport across the blood-brain barrier through a mechanism that other magnesium salts do not replicate.
The Sleep–Cognition Dual Mechanism
Magnesium plays a documented role in sleep architecture — specifically in promoting deeper slow-wave sleep stages where the most critical memory consolidation occurs. MgT’s evening timing recommendation is not merely conventional — it is mechanistically optimal. Better sleep architecture means more efficient overnight consolidation of daytime learning; more efficient consolidation means that the synaptic plasticity improvements MgT drives during waking hours are more completely converted into durable long-term memories. The sleep benefit and the cognitive benefit are not independent effects — they are mechanistically linked through the memory consolidation process.
Magnesium L-Threonate — The Numbers
Magnesium L-Threonate — Evidence Hierarchy
🟢 Strong human RCTs | 🟡 Moderate evidence | 🔴 Preliminary only
Clinical Evidence: The Landmark Trials
Mechanistic Foundation — MIT Neuron Publication
Slutsky et al. (2010) — Synaptic Density and Memory Enhancement
Published in Neuron — one of the most prestigious neuroscience journals — this MIT study established the foundational mechanistic case for MgT. Elevating brain magnesium concentrations using Magnesium L-Threonate in animal models produced a significant increase in hippocampal synaptic density (number of functional synaptic connections) and improvements in both short-term and long-term memory. The hippocampal synaptic density finding is the most important mechanistic result: more synaptic connections means greater structural capacity for memory encoding, storage, and retrieval. This study attracted the funding for subsequent human clinical trials by demonstrating a mechanistically coherent, structurally verifiable cognitive enhancement pathway unique to MgT.
Landmark Human RCT — Age-Related Cognitive Decline
Liu et al. (2016) — 9 Years of Cognitive Decline Reversed
51 adults aged 50–70 with subjective memory complaints were randomised to 2,000mg Magtein® daily or placebo for 12 weeks in a double-blind design. The Magtein® group showed significant cognitive improvements across multiple domains — with the overall cognitive composite score improvement corresponding to an estimated reversal of approximately 9 years of age-related cognitive decline. Executive function and working memory showed the most pronounced improvements. Importantly, no serious adverse effects were reported, and compliance was high throughout the 12-week period. The effect size of this reversal — roughly 9 years in 12 weeks — is among the most striking findings in any nootropic clinical trial and was the primary reason this compound attracted sustained scientific attention beyond the initial MIT mechanistic study.
Liu G, et al. J Alzheimers Dis. 2016;49(4):971–990. PMID 27642901
RCT — Healthy Adults, All Ages
Zhang et al. (2022) — Magtein® in Healthy Chinese Adults (18–65)
109 healthy adults aged 18–65 were randomised to a Magtein®-based formula (2g daily) or placebo for 30 days. The Magtein® group showed statistically significant improvements across all five subcategories of the Clinical Memory Test — the standard cognitive evaluation tool used in Chinese hospitals and research institutes — as well as the overall Memory Quotient score. Critically, older participants showed greater improvement than younger participants, consistent with the hypothesis that cognitive benefit scales with the degree of underlying deficiency. This trial established that MgT’s cognitive benefits are not limited to cognitively impaired or elderly populations — healthy adults show measurable improvements within 30 days.
Magtein® vs Generic MgT — Why This Distinction Matters
The clinical evidence for MgT was generated using Magtein® — the branded, patented form of Magnesium L-Threonate developed at MIT and licensed to Amen Clinics for manufacturing. Magtein® has a specific particle size, purity specification, and production process that were used in every human trial cited in this article. Generic “magnesium L-threonate” powder from unverified manufacturers has no confirmed clinical equivalence to Magtein® — the threonate salt chemistry may be nominally identical, but particle size, solubility, and impurity profile can affect bioavailability in ways that the clinical trials did not test.
Practical guidance: When selecting MgT, confirm that the product specifies Magtein® on the label — this indicates the branded form used in clinical research. Products that list only “magnesium L-threonate” without the Magtein® trademark may be using generic raw material with unverified bioavailability equivalence. The premium is meaningful here unlike in commodity supplements like creatine monohydrate where the active compound is chemically simple and the form distinction is minimal.
How Readers Are Using Magnesium L-Threonate
Composite profiles based on reader-reported experiences. Individual results vary.
Martin, 62
Retired GP, concerned about age-related memory
“I started after reading the Liu et al. trial. I’m 62 and within the age profile studied. At 12 weeks, my performance on the MOCA test had improved by 2 points — which sounds modest but is clinically meaningful at my age. The sleep improvement was the first thing I noticed — about week 3. Deeper sleep, more vivid dreams, waking feeling more rested. The cognitive improvement followed over months. My wife — who doesn’t know I’m supplementing — independently noted I seem ‘sharper.’ That’s the result that matters.”
Protocol: 2,000mg Magtein® nightly with dinner · 12 weeks continuous · MOCA +2 points · Sleep improvement wk 3
Priya, 34
Data scientist, plant-based diet
“I already take magnesium glycinate for sleep and muscle recovery. I added MgT specifically for the brain benefits — they’re not redundant compounds. The glycinate handles my systemic magnesium status and sleep onset; the MgT handles brain-specific magnesium. The combination improved my HRV (measured via Oura Ring) more than either alone. I notice the difference in cognitive flexibility during complex modelling sessions — I hold problem spaces together better. I can’t isolate the MgT specifically but the stack change correlates clearly.”
Protocol: MgT 2,000mg + Magnesium Glycinate 200mg — separate mechanisms, combined nightly · HRV improved
James, 47
Barrister, demands on verbal precision
“I came to this through the sleep angle — I was getting 7+ hours but the quality was poor and I woke tired. MgT changed the character of my sleep, not the duration. I wake feeling genuinely rested in a way I wasn’t before. The cognitive benefit I notice most is what I’d call executive agility — the ability to hold multiple threads simultaneously in complex legal arguments. That specific quality improved over about 8 weeks. My chambers colleagues use it too now after I mentioned it.”
Protocol: 2,000mg Magtein® 30 min before bed · 8 weeks to executive function improvement · Sleep quality primary
Sasha, 28
PhD student, neuroscience
“I added MgT specifically because I’m already using Bacopa and Alpha-GPC — and the NMDA receptor story made mechanistic sense to me as someone who studies synaptic plasticity. Creatine gives me energy buffer; Bacopa gives me AChE inhibition and dendritic branching; Alpha-GPC gives me ACh substrate; MgT ensures my NMDA gating is optimally tuned. These are non-overlapping mechanisms. It’s the most intellectually satisfying stack I’ve designed. Whether my productivity data supports it is harder to say — too many variables.”
Protocol: MgT 2,000mg nightly + Bacopa + Alpha-GPC + Creatine — complete mechanistic stack architecture
The NeuroEdge Synaptic Density Protocol
MgT as the NMDA receptor and synaptic plasticity layer — ensuring the cellular machinery for memory encoding is operating at optimal magnesium-tuned sensitivity. The most mechanistically underappreciated addition to any advanced cognitive protocol. Peter Benson’s nightly MgT protocol, 3+ years continuous. Updated June 2026.
2,000mg Magtein® nightly — 30–60 minutes before sleep. Evening timing activates both the cognitive and sleep benefit simultaneously. Source: Performance Lab Sleep contains Magtein® alongside Montmorency cherry and L-tryptophan for the complete sleep-cognitive stack.
Specify Magtein® on the label — not just “magnesium L-threonate.” The clinical trials used Magtein® specifically. Generic MgT powder has no confirmed clinical equivalence. This is the one category where the branded form matters for evidence alignment.
MgT and magnesium glycinate are not redundant — different objectives and mechanisms. Glycinate addresses systemic magnesium status, muscle relaxation, and sleep onset. MgT addresses brain-specific magnesium and NMDA receptor tuning. Both can be taken together — track total elemental magnesium across all forms against the NIH upper tolerable intake (350mg supplemental elemental Mg daily).
MgT sits in the evening / sleep window alongside Ashwagandha (cortisol/sleep quality) and DHA (structural substrate). Morning compounds (Alpha-GPC, Bacopa, Creatine) are daytime-performance compounds. MgT spans both: daytime NMDA tuning + overnight consolidation enhancement.
Peter’s Testing Notes — Magnesium L-Threonate
3+ years continuous · Updated June 2026
I introduced Magnesium L-Threonate into my protocol three years ago — later than most of the other compounds in this series, which I attribute to an initial dismissiveness about magnesium as a cognitive compound. The Slutsky et al. Neuron paper changed my assessment: the hippocampal synaptic density finding is not a marginal improvement claim — it is a structural neuroplasticity mechanism that would theoretically amplify the effectiveness of every other neuroplasticity compound in the protocol. Once that mechanistic picture was clear, adding MgT was an obvious decision. I source exclusively from Performance Lab Sleep, which combines Magtein® with Montmorency cherry (melatonin precursor) and L-tryptophan — taken 30–45 minutes before sleep.
The first detectable change was in sleep quality — not sleep duration but sleep depth. By week 3 I noticed subjectively deeper sleep and more vivid, structured dream recall (which correlates with REM depth in my experience). By week 6, my Creyos executive function scores had improved by approximately 11% above pre-MgT baseline on matched-condition testing days. I cannot separate the MgT contribution from general protocol maturation over those six weeks — but the timing correlation and the mechanistic plausibility make MgT the most credible candidate for that specific executive function improvement.
The compound I consider most underappreciated in this entire series — not because it produces the most dramatic acute effects, but because it addresses the NMDA receptor substrate on which every other neuroplasticity compound I take depends. Bacopa drives dendritic branching: the new synapses benefit from MgT’s optimal NMDA gating. Lion’s Mane increases NGF for cholinergic neuron health: those cholinergic neurons use NMDA receptor-dependent LTP for synaptic strengthening. DHA ensures the neuronal membranes those receptors sit in are optimally fluid. These are mechanistically non-overlapping layers, and MgT is the one that is most commonly missing from otherwise sophisticated cognitive protocols.
Sourcing Standards
The most important sourcing decision for MgT is confirming Magtein® certification — not simply “magnesium L-threonate.” Check the supplement facts panel or brand website for explicit Magtein® trademark. After confirming Magtein®, the secondary consideration is the companion formula: MgT taken as part of a sleep-focused formula (alongside Montmorency cherry, L-tryptophan, or 5-HTP) amplifies the overnight consolidation mechanism through multiple synergistic pathways.
Performance Lab Sleep — Magtein® + Montmorency Cherry + Tryptophan
My nightly protocol for 3+ years. Combines Magtein® with Montmorency cherry concentrate (natural source of melatonin precursors) and L-tryptophan (serotonin/melatonin pathway support). The formula addresses all three layers of sleep-based cognitive enhancement: brain magnesium for NMDA tuning, melatonin pathway for sleep onset, tryptophan for mood-regulated consolidation. Performance Lab uses Magtein® specifically — confirmed trademark on the label and product page.
Magtein® confirmed · With Montmorency cherry + L-tryptophan · Nightly sleep protocol · Ubernet 30% commission
BiOptimizers — Magnesium Breakthrough (7 Forms Including MgT)
Magnesium Breakthrough by BiOptimizers provides all 7 forms of magnesium in one product — including Magtein® (MgT) alongside glycinate, malate, taurate, and others. For users who want to address both systemic magnesium deficiency and brain-specific magnesium simultaneously in one product, this is the most comprehensive approach. The MgT dose per serving is lower than standalone Magtein® products — users specifically targeting the 2,000mg clinical dose may need to supplement additionally.
7 magnesium forms including Magtein® · Comprehensive systemic + brain coverage · Clickbank neurohq ID · 40%+ commission
Key Takeaways — Magnesium L-Threonate
MgT is the only magnesium form that meaningfully raises brain magnesium — even a 150–200% plasma magnesium increase from standard forms only raises CSF magnesium by 10–19%. The threonate carrier enables active transport across the blood-brain barrier that other forms cannot achieve.
Specify Magtein® — not just “magnesium L-threonate” — the clinical evidence was generated with the Magtein® branded form. Generic MgT has no confirmed clinical equivalence. This is the one category where the branded form specification directly aligns with the evidence base.
Evening timing is optimal — not just conventional — MgT’s sleep quality benefit and its cognitive mechanism are mechanistically linked through overnight memory consolidation. Taking it before sleep activates both pathways simultaneously.
MgT and magnesium glycinate are not redundant — they serve different objectives. Glycinate for systemic deficiency, muscle relaxation, and sleep onset. MgT for brain-specific magnesium and NMDA receptor tuning. Both can and should be combined for users addressing both objectives.
48% magnesium deficiency prevalence means most users are not starting from an optimal baseline — for the majority of Western adults, MgT supplementation is not marginal optimisation but genuine restoration of a deficit that impairs the NMDA receptor mechanism underlying all forms of synaptic plasticity and memory formation.
Magnesium L-Threonate — FAQ
What makes Magnesium L-Threonate different from other magnesium forms?
The blood-brain barrier strictly regulates magnesium entry into the CNS. Standard magnesium supplements — glycinate, oxide, citrate, malate — raise plasma magnesium effectively but cross the blood-brain barrier poorly. Research has confirmed that even a 150–200% increase in plasma magnesium only raises CSF magnesium by 10–19%. The threonate carrier in MgT appears to facilitate active transport across this barrier, uniquely enabling meaningful increases in brain magnesium concentrations. This is not a marketing claim — it was the experimental finding that drove the MIT research and subsequent clinical trials.
Can I take MgT during the day instead of at night?
You can, but evening timing is mechanistically superior. The sleep benefit — which works through deepening slow-wave sleep to enhance overnight memory consolidation — only operates during sleep. Taking MgT in the morning loses the sleep-quality component of its dual mechanism. Some users find daytime MgT produces mild relaxation or slight sedation — for those sensitive to magnesium’s calming effects, morning dosing may affect alertness. Evening is the recommended and mechanistically optimal timing.
How long before I notice effects?
Sleep quality improvements often appear within 2–4 weeks — the sleep benefit is typically the first signal. Cognitive improvements, particularly in executive function and working memory, are documented at 12 weeks in the Liu et al. trial. Brain magnesium concentrations build progressively with daily supplementation — the NMDA receptor and synaptic plasticity effects are cumulative structural changes, not acute pharmacological events. Evaluate sleep benefits at 4 weeks; cognitive benefits at 12 weeks minimum.
Should I also take regular magnesium glycinate?
Yes, if you have systemic magnesium deficiency or want to address peripheral magnesium needs (muscle relaxation, sleep onset, general nervous system function). MgT addresses brain-specific magnesium; glycinate addresses systemic magnesium. They serve different purposes and can be combined. Track total elemental magnesium across both forms — the NIH upper tolerable intake for supplemental magnesium is 350mg elemental magnesium daily. MgT provides approximately 144mg elemental magnesium per 2,000mg Magtein® dose.
Does MgT work if I’m not magnesium deficient?
Possibly, though effects are likely smaller. Standard serum magnesium testing may not accurately reflect brain magnesium status — the brain maintains magnesium concentrations through active transport mechanisms that can become impaired with age even when serum levels appear normal. Research finding cognitive benefits in healthy adults without baseline deficiency suggests that elevating brain magnesium above typical levels may produce benefits even without clinically measurable systemic deficiency. The largest benefits are most consistently documented in older adults and those with poor dietary magnesium intake.
7 Days to a Sharper Brain
Peter Benson’s personal daily protocol, rebuilt from 18 years of testing
The complete evening sleep and recovery stack — where MgT fits, why the timing matters, and how it amplifies everything else you’re doing in your cognitive protocol during overnight consolidation.
Join 2,000+ readers optimising their cognitive performance. Unsubscribe anytime.
Scientific References
- Slutsky I, et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron, 65(2):165–177. PMID 20152124
- Liu G, et al. (2016). Efficacy and safety of MMFS-01, a synapse density enhancer, for treating cognitive impairment in older adults: a randomized, double-blind, placebo-controlled trial. Journal of Alzheimer’s Disease, 49(4):971–990. PMID 27642901
- Zhang C, et al. (2022). A Magtein®, Magnesium L-Threonate-based formula improves brain cognitive functions in healthy Chinese adults. Nutrients, 14(24):5235. PMC9786204
- Abbasi B, et al. (2012). The effect of magnesium supplementation on primary insomnia in elderly: a double-blind placebo-controlled clinical trial. Journal of Research in Medical Sciences, 17(12):1161–1169. PMID 23853635
- Killilea DW & Ames BN. (2008). Magnesium deficiency accelerates cellular senescence in cultured human fibroblasts. PNAS, 105(15):5768–5773. PMID 18378903
- Rosanoff A, et al. (2012). Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutrition Reviews, 70(3):153–164. PMID 22364157
- Maier JAM, et al. (2012). Low magnesium promotes endothelial cell dysfunction. Magnesium Research, 25(1):12–21. PMID 22510792
- National Institutes of Health — Office of Dietary Supplements. Magnesium Fact Sheet for Health Professionals. NIH ODS
Peter Benson
Cognitive Enhancement Researcher | 18+ Years Independent Research
Peter Benson has spent 18 years researching cognitive enhancement through personal experimentation and systematic review of the scientific literature. He considers Magnesium L-Threonate the most underappreciated compound in any serious intermediate cognitive protocol, and has used Magtein® nightly for 3+ years as the NMDA receptor and synaptic plasticity layer of his complete cognitive stack.
Last reviewed: June 2026 | Educational content only. Not medical advice.